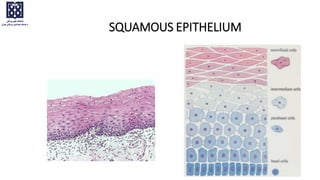
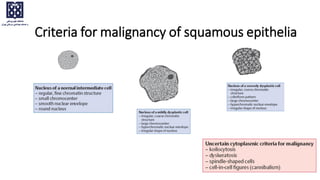
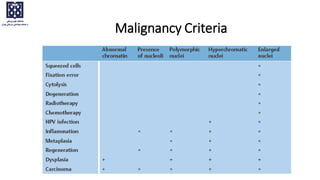
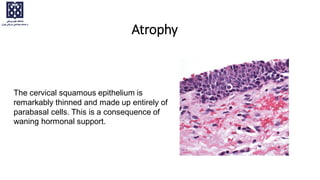
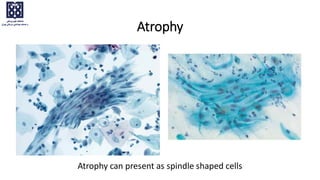
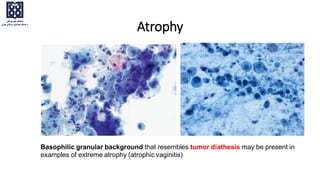
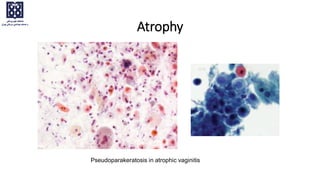
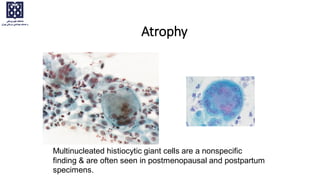
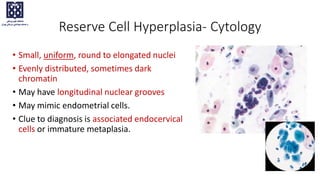
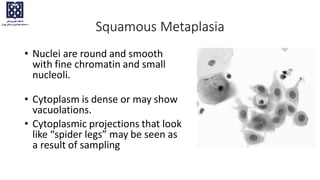
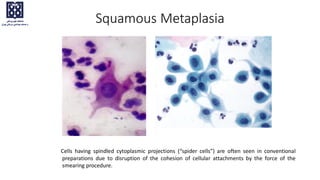
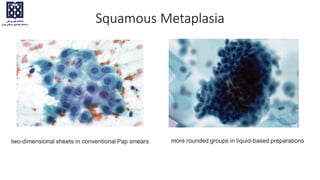
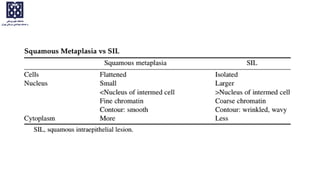
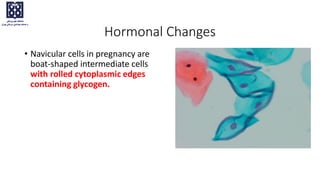
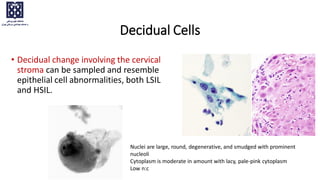
This document discusses features evaluated in Pap tests and provides explanations of common non-neoplastic cellular variations seen in Pap tests, including atrophy, keratotic changes, metaplasia, and hormonal changes. It describes criteria for malignancy of squamous epithelia and notes that no single criteria is absolutely reliable, and the likelihood of malignancy increases with the number of criteria present.






























![Cytopathology Of Cerebrospinal Fluid[1]Power Point](https://cdn.slidesharecdn.com/ss_thumbnails/cytopathologyofcerebrospinalfluid1power-point-1230479978520994-2-thumbnail.jpg?width=640&height=640&fit=bounds)








































