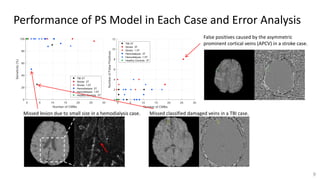
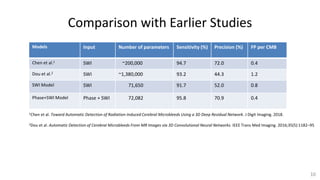
This document describes a study using deep learning to detect cerebral microbleeds (CMBs) from susceptibility weighted imaging (SWI). It found that using both SWI and phase images as inputs to a neural network led to better performance than SWI alone. The best model achieved 95.8% sensitivity and 70.9% precision, similar to human experts. This outperformed previous studies and demonstrated the potential of deep learning for medical image analysis tasks.
![Data Information and Pre-processing
4
Hemodialysis TBI Stroke Normal Control Total
Training 72 (756)a 80 (522) 2 (2) 0 154 (1280)
Validation 15 (160) 8 (33) 2 (0) 0 25 (193)
Test 13 (95) 9 (14) 9 (59) 10 (0) 41 (168)
Data
Splitting
B0 (T) TE (ms) TR (ms) FA (o) In-plane
Resolution (mm2)
Slice Thickness
(mm)
1.5 or 3 40@1.5T;
20@3T
49 or 50 @ 1.5T;
27 to 34 @ 3T
12 or 15 0.5x0.5 to
0.54x1.07
1.2 to 2.65
Imaging
Parameters
aNumber of Cases (Number of CMBs)
Bias-field
Correction
(for magnitude)
Registration
(Magnitude with
MNI-152 template)
Generate
SWI&QSMb
Interpolation
(to 0.5mm
isotropic)
Intensity
Normalization
(to [-1, 1])
Pre-processing
bQSM: quantitative susceptibility mapping](https://image.slidesharecdn.com/cmb-slideshare-20190523-190528164101/85/Cerebral-Microbleed-Detection-using-Susceptibility-Weighted-Imaging-and-Deep-Learning-6-320.jpg)