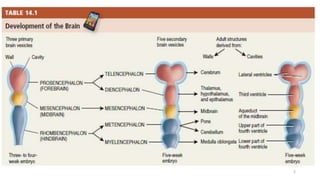
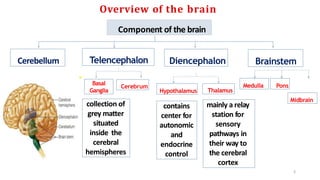
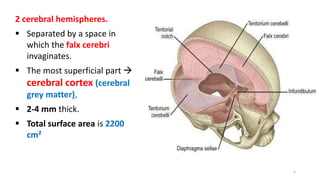
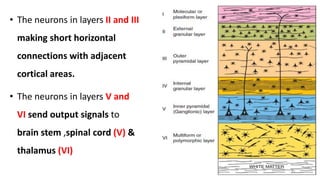
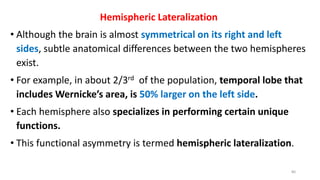
The document summarizes the anatomy and function of the cerebral cortex. It describes the lobes, layers, and Brodmann areas of the cortex. The primary functions of the frontal lobe are motor control and planning located in the precentral cortex. The prefrontal cortex is involved in working memory, personality, and social behavior. Sensory processing occurs in the primary sensory areas, while association areas integrate information between regions for functions like language, vision, and emotion.


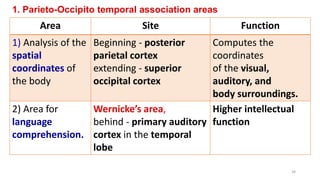
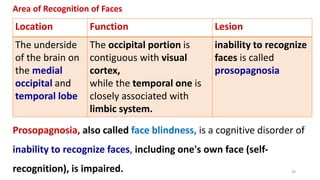
![2. Prefrontal Association Area -Broca’s Area
Definition Function Lesion
Broca’s Area [44,45]
located partly in the
posterior lateral
prefrontal cortex
and partly in the
premotor area
Provides the Neural
Circuitry for Word
Formation.
Broca's aphasia or
expressive aphasia.
--difficulty in forming
words and producing
speech but do not
struggle with
comprehension
37](https://image.slidesharecdn.com/cerebralcortex-29dec-231229052945-d484693d/85/CEREBRAL-CORTEX-PHYSIOLOGY-FUNCTIONS-AND-LESIONS-29-DEC-pptx-37-320.jpg)
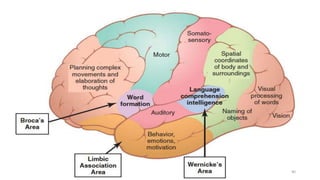
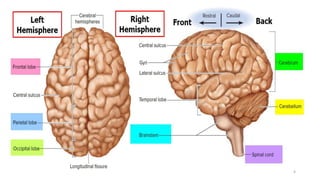
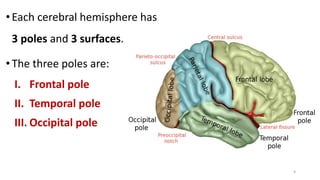
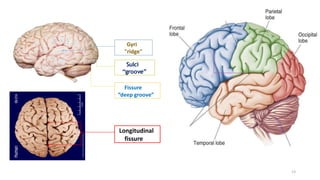
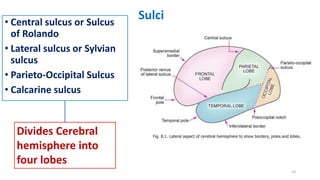
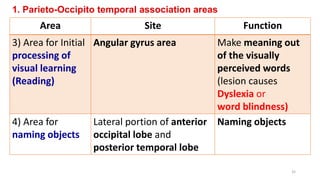
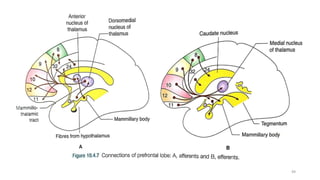
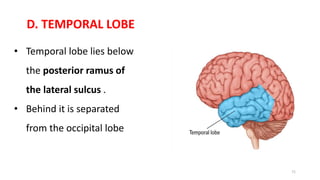
![[A] FRONTAL LOBE
• Lies in front of the central sulcus and above the posterior ramus of the
lateral sulcus .
• frontal lobe is subdivided into two main areas:
1. Precentral cortex and
2. Prefrontal cortex.
I. Precentral cortex
• Posterior part of the frontal lobe .
• Excitomotor area of cortex.
41](https://image.slidesharecdn.com/cerebralcortex-29dec-231229052945-d484693d/85/CEREBRAL-CORTEX-PHYSIOLOGY-FUNCTIONS-AND-LESIONS-29-DEC-pptx-41-320.jpg)
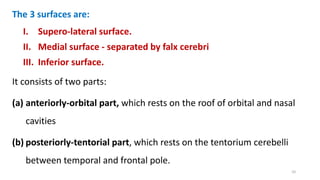
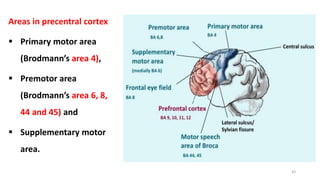
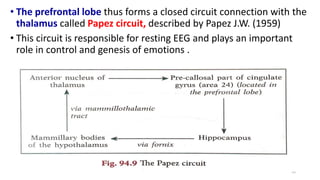
![[A] FRONTAL LOBE
42](https://image.slidesharecdn.com/cerebralcortex-29dec-231229052945-d484693d/85/CEREBRAL-CORTEX-PHYSIOLOGY-FUNCTIONS-AND-LESIONS-29-DEC-pptx-42-320.jpg)
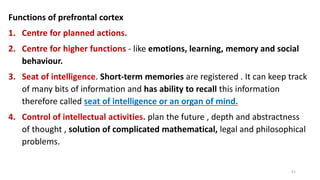
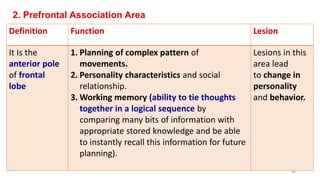
![APPLIED ASPECTS
Frontal lobe syndrome
• Due to injury or ablation of prefrontal cortex.
• Prefrontal leucotomy, i.e. cutting the connection between the
thalamus and prefrontal lobe
• Prefrontal lobectomy (extirpation- to destroy completely )
• In the past, these operations were performed in patients with
severe mental illness.[not now]
52](https://image.slidesharecdn.com/cerebralcortex-29dec-231229052945-d484693d/85/CEREBRAL-CORTEX-PHYSIOLOGY-FUNCTIONS-AND-LESIONS-29-DEC-pptx-52-320.jpg)
![Connections -It is well connected with:
1. Thalamus (LGN)
2. Frontal eye field (area 8)
3. Pineal body
4. Tectum-Superior colliculus [midbrain]
5. Hypothalamus
6. Limbic lobe
7. Posterior parietal cortex area 78.
8. Temporal lobe-Superior and inferior temporal gyri areas 22, 21, 20
and 37
68](https://image.slidesharecdn.com/cerebralcortex-29dec-231229052945-d484693d/85/CEREBRAL-CORTEX-PHYSIOLOGY-FUNCTIONS-AND-LESIONS-29-DEC-pptx-68-320.jpg)
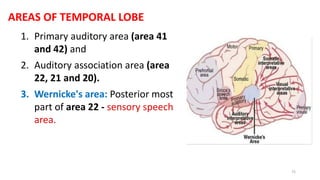
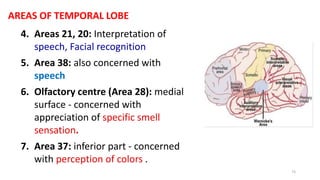
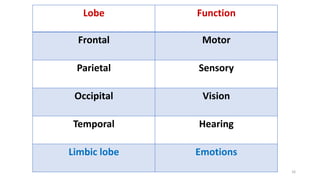
![Functions
1. It has the centre for hearing [Area 41]
2. Interpretation of various sounds.
3. Language comprehension and other higher intellectual functions
[Areas 42 and 22 ].
4. Recent memory.
5. Facial recognition (areas 21 and 20).
6. Color vision (area 37).
7. Participates in olfaction (area 28).
75](https://image.slidesharecdn.com/cerebralcortex-29dec-231229052945-d484693d/85/CEREBRAL-CORTEX-PHYSIOLOGY-FUNCTIONS-AND-LESIONS-29-DEC-pptx-75-320.jpg)
























































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)

















