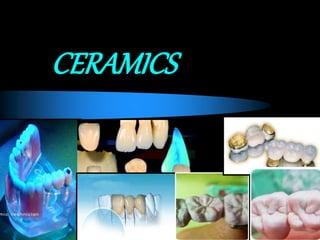
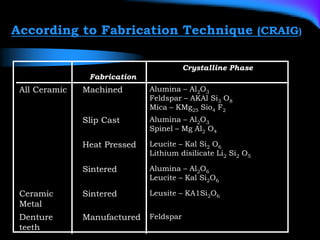
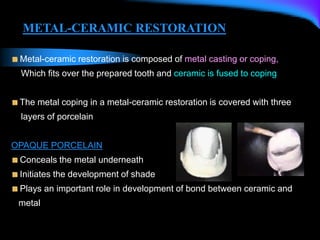
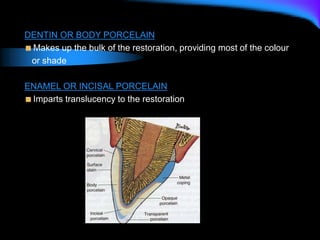
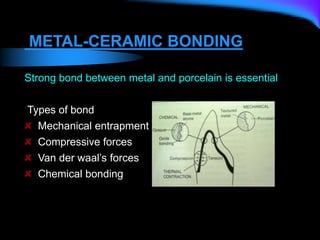
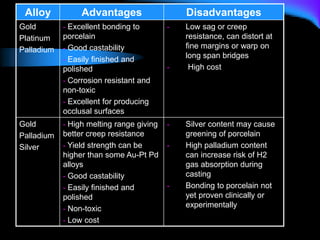
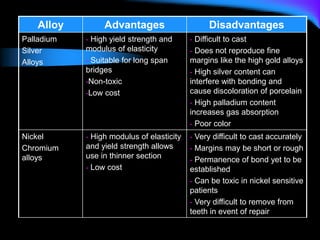
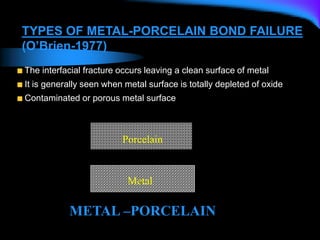
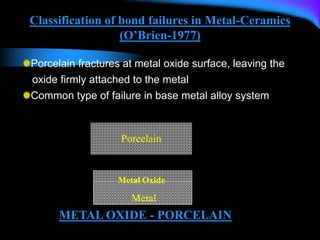
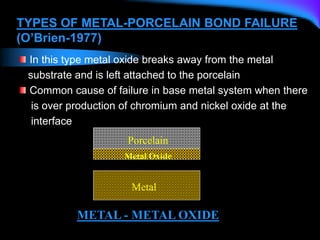
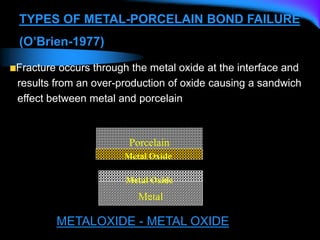
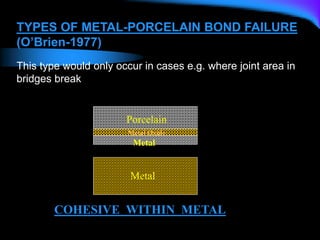
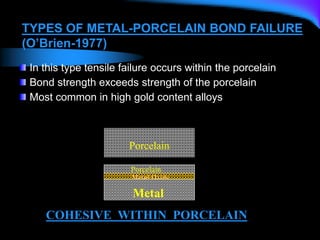
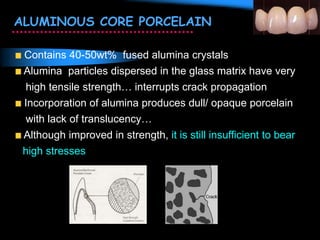
Ceramics are inorganic, non-metallic materials formed from chemical and biochemical stable substances. Dental ceramics contain a glassy matrix reinforced by crystalline structures such as leucite, alumina, and silica. Dental porcelains are composed of feldspar, silica, and kaolin, which are blended and fired to form the ceramic. Metal-ceramic restorations consist of a metal coping covered with opaque, dentin, and enamel porcelain layers that are bonded to the metal through mechanical interlocking and chemical bonding between metal oxide layers and the ceramic.


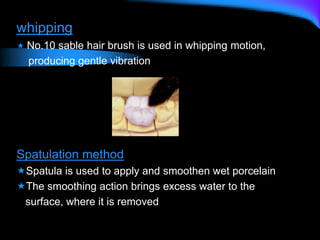








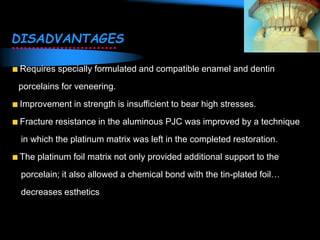

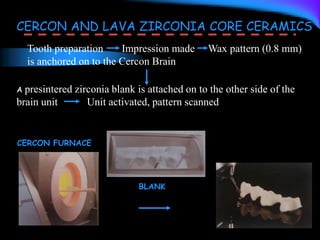
![CAD CAM
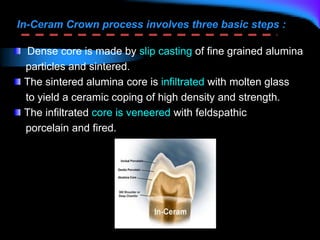
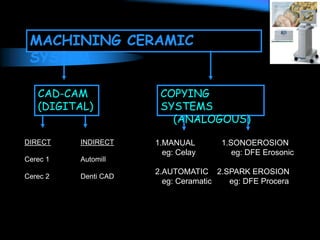
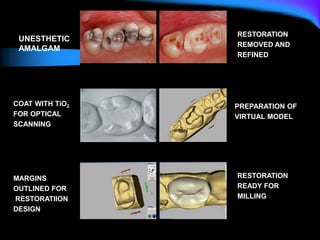
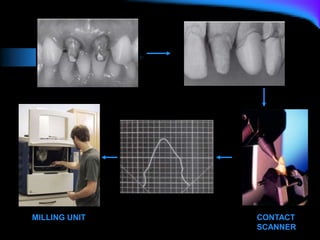
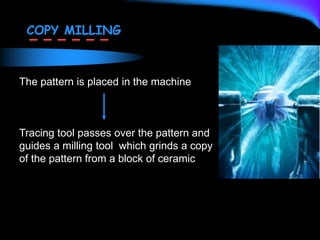
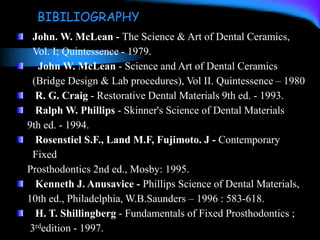
Uses digital information about the tooth preparation or a pattern of
the restoration to provide a computer-aided design (CAD) on the
video monitor for inspection and modification.
The image is the reference for designing restoration on video monitor.
Once the 3-D image for the restoration design is accepted, computer
translates the image into a set of instructions to guide a milling tool
(computer-assisted manufacturing [CAM]) in cutting the restoration
from block of material.](https://image.slidesharecdn.com/ceramics-230922071115-eec65551/85/ceramics-ppt-149-320.jpg)
















![Dental Casting alloys [DENTAL MATERIALS]](https://cdn.slidesharecdn.com/ss_thumbnails/castingalloysbp-200331155134-thumbnail.jpg?width=640&height=640&fit=bounds)
















































![biomechanicsfinalppt1-240820043808-0bcee79a [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/biomechanicsfinalppt1-240820043808-0bcee79aautosaved-250319054528-6f847c97-thumbnail.jpg?width=640&height=640&fit=bounds)


























