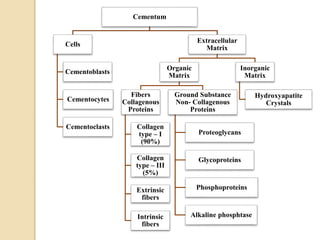
This document provides an overview of cementum, including its physical characteristics, composition, functions, classification, locations, abnormalities, and more. Cementum is the avascular, mineralized tissue covering tooth roots. It is composed of cells, collagen fibers, and hydroxyapatite crystals. Cementum functions to provide anchorage for fibers attaching teeth to bone and aids in adaptation and repair. It can be classified based on presence of cells, fiber origin, location, and matrix composition. Abnormalities include aplasia, hypoplasia, and hypercementosis.