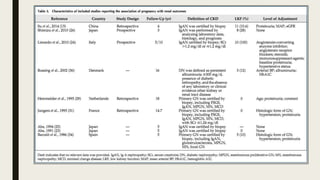
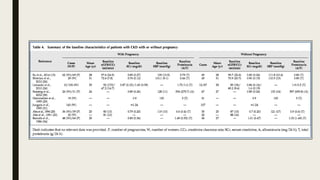
1) This study conducted a systematic review and meta-analysis of 23 studies to examine the effects of chronic kidney disease (CKD) on pregnancy outcomes and the effects of pregnancy on renal outcomes in women with CKD.
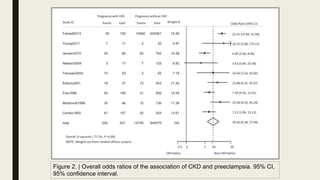
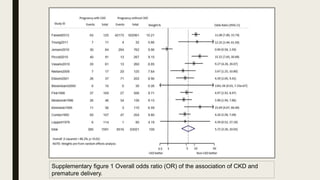
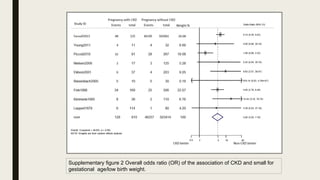
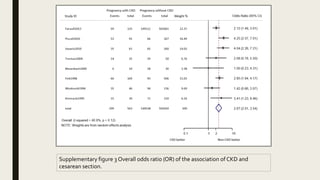
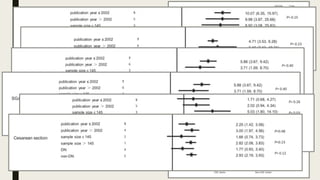
2) The results showed that women with CKD faced significantly higher risks of adverse pregnancy outcomes like preeclampsia, premature birth, and small-for-gestational-age babies compared to women without CKD.
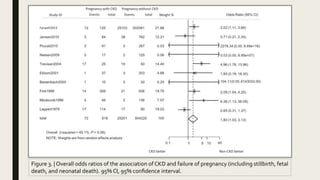
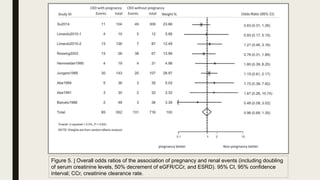
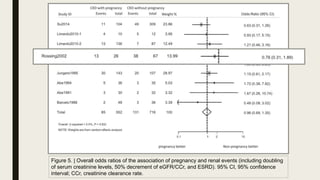
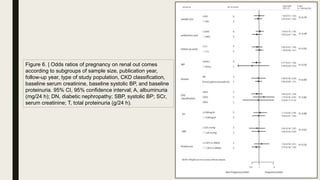
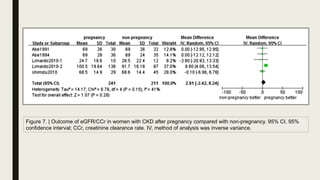
3) However, the study found no evidence that pregnancy led to worsening of renal outcomes in women with CKD compared to non-pregnant women with CKD. Pregnancy did not appear to negatively impact kidney function or progression to kidney failure.