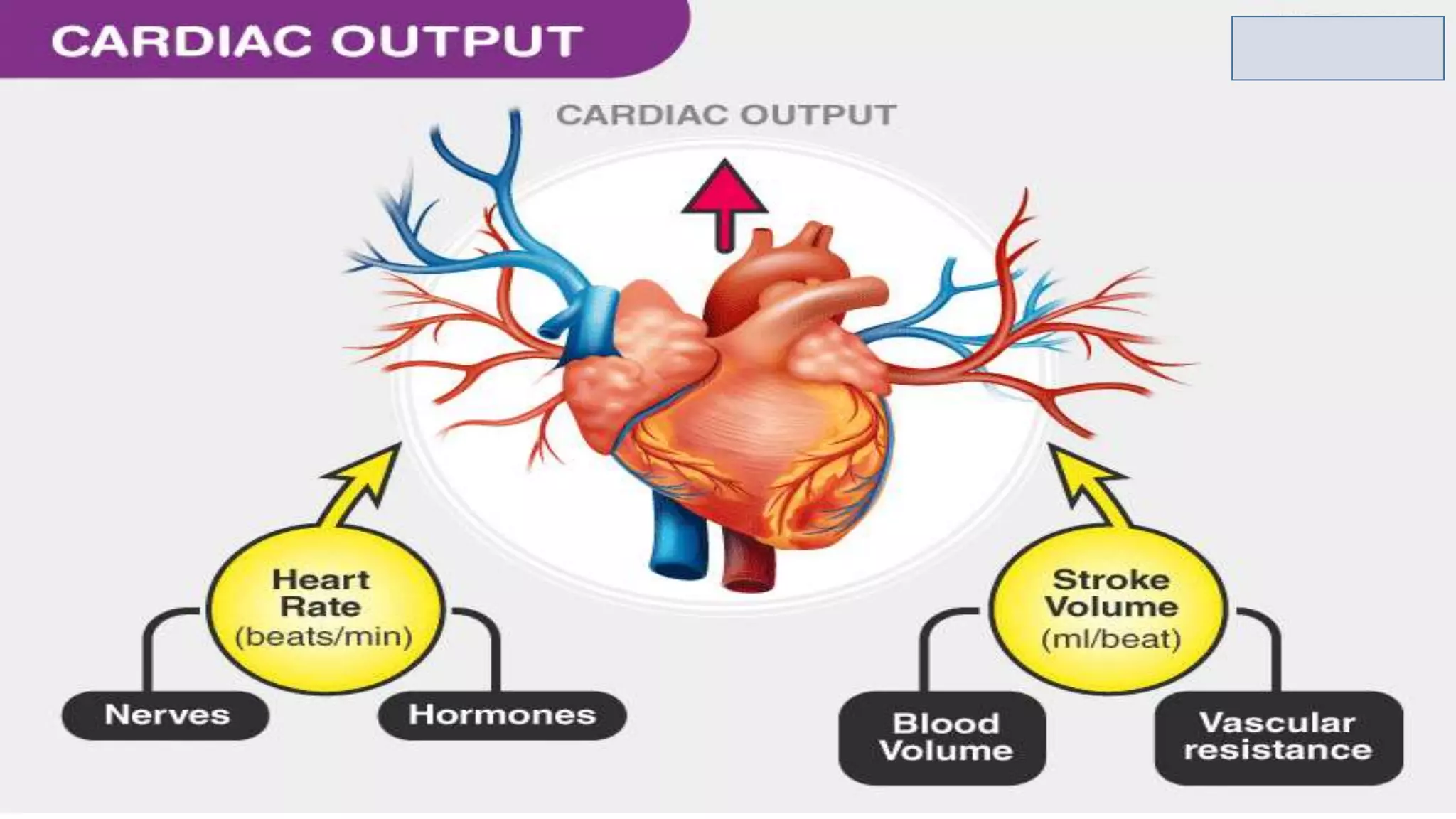
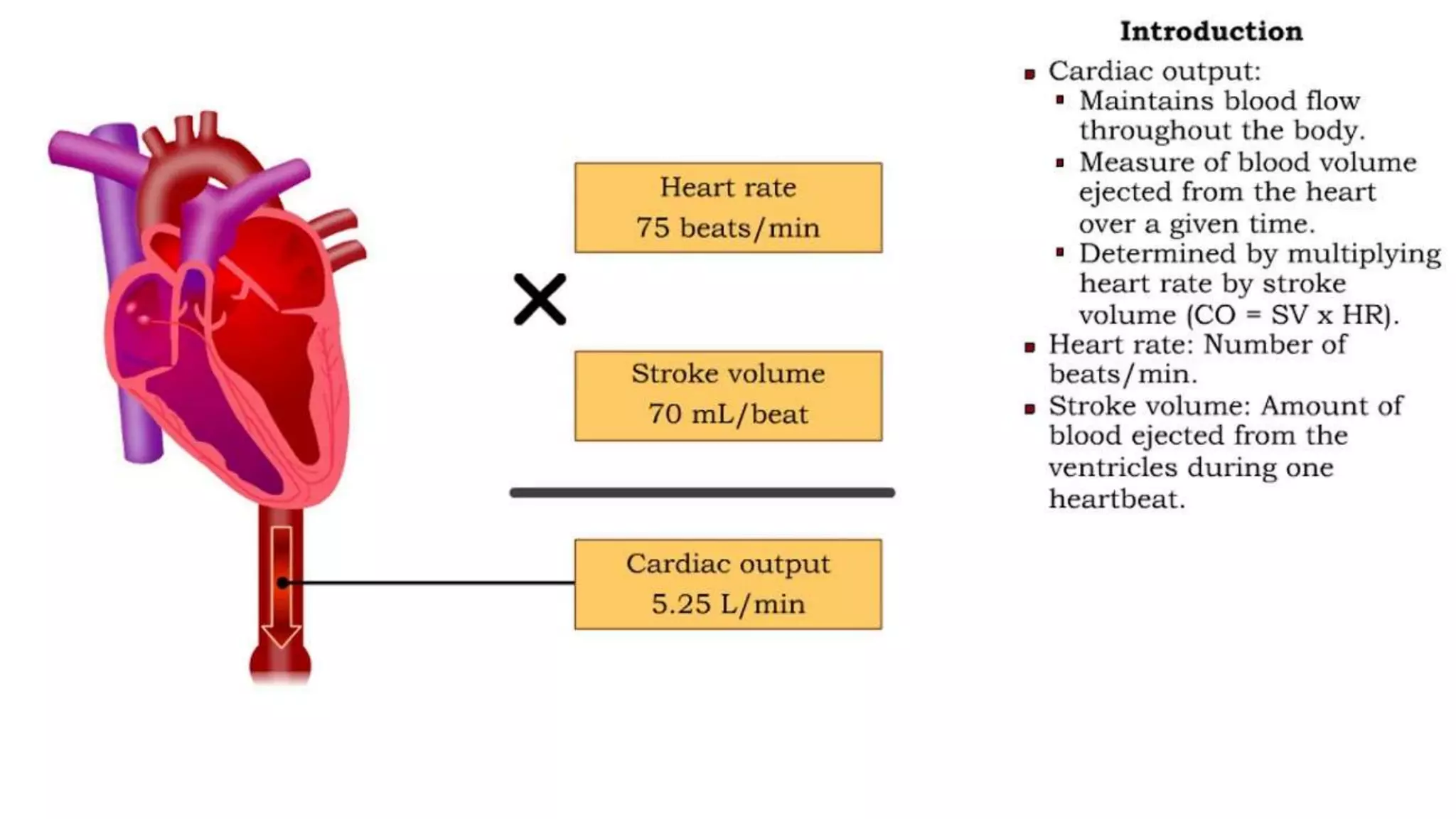
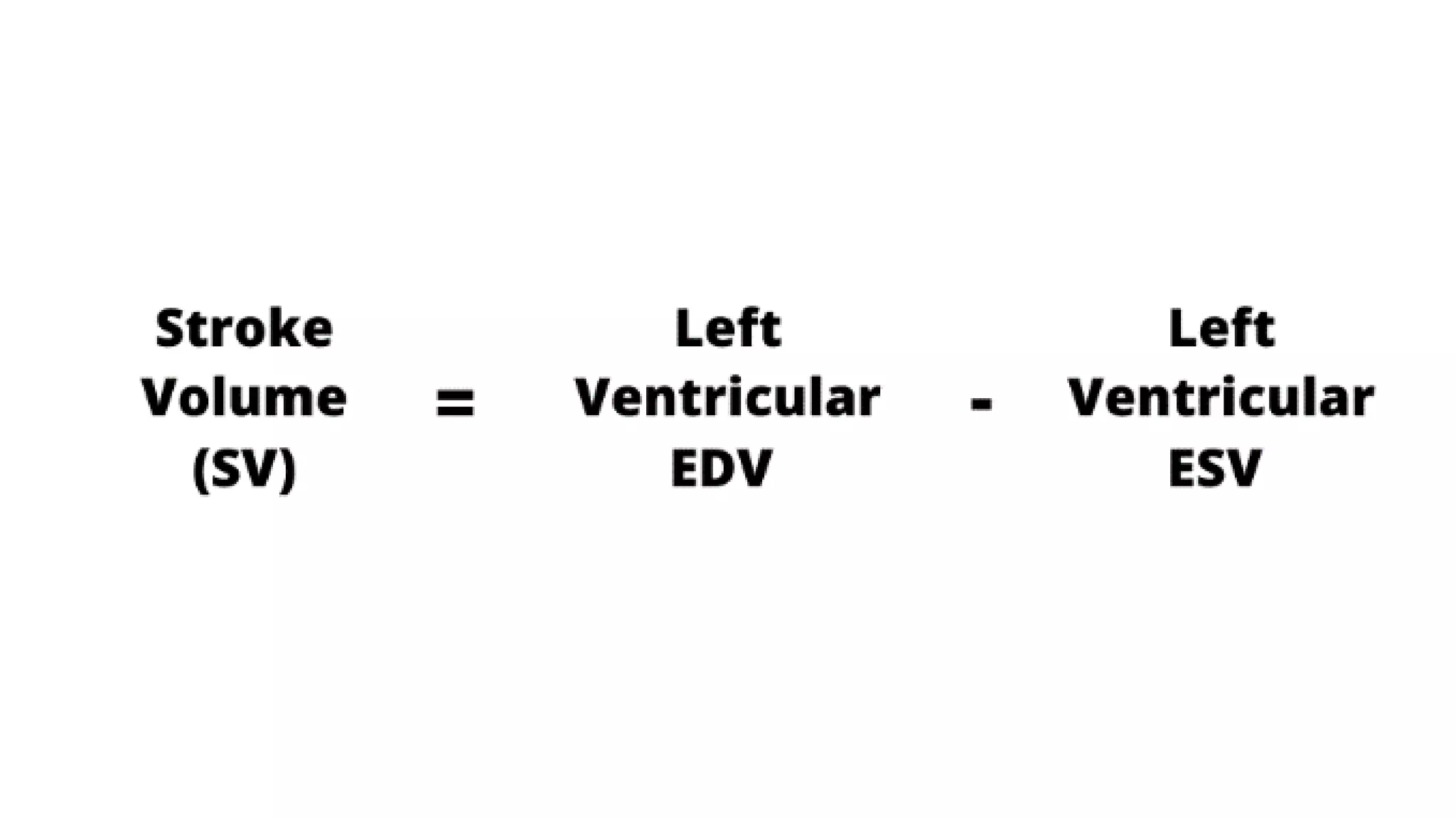
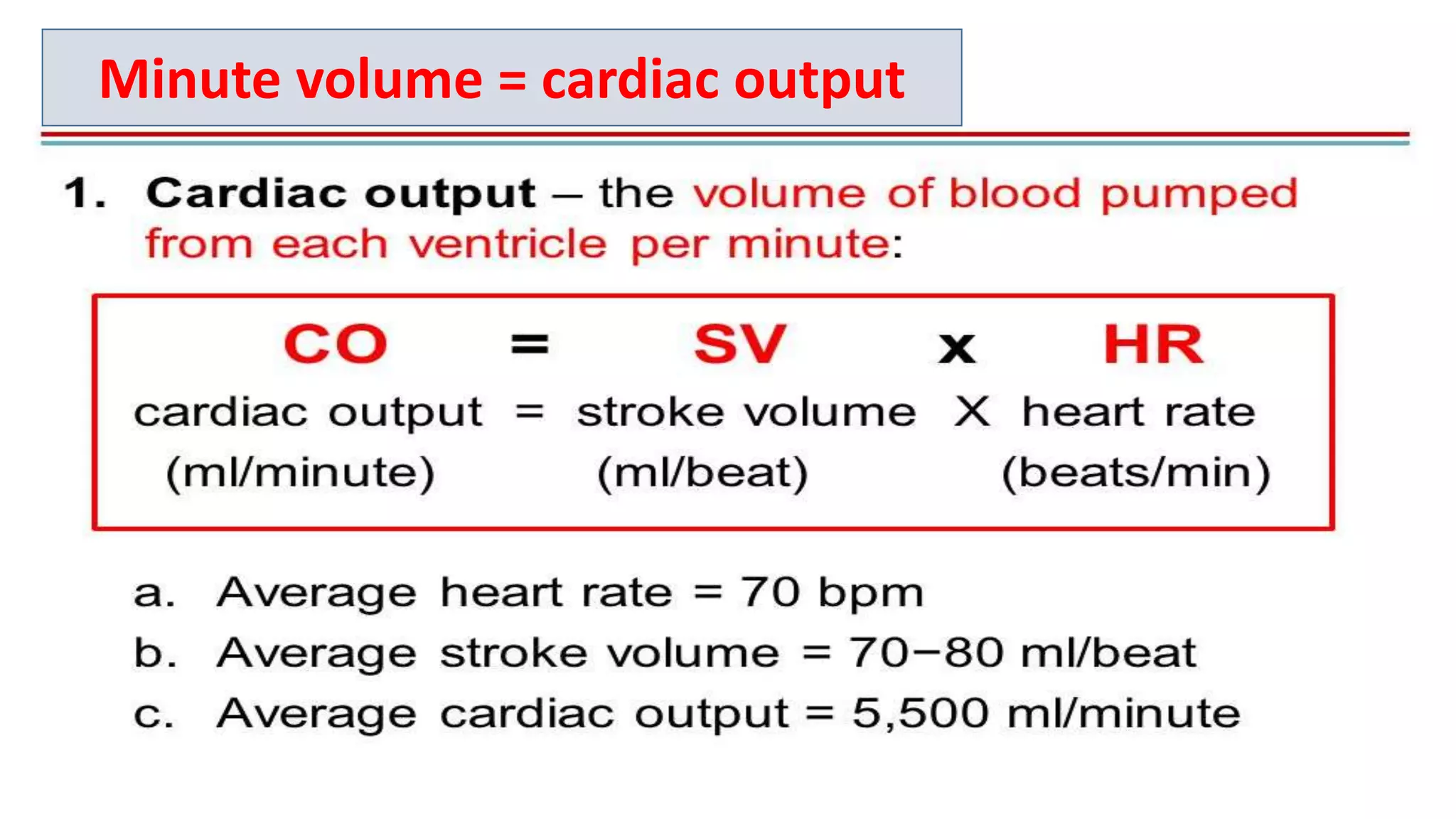
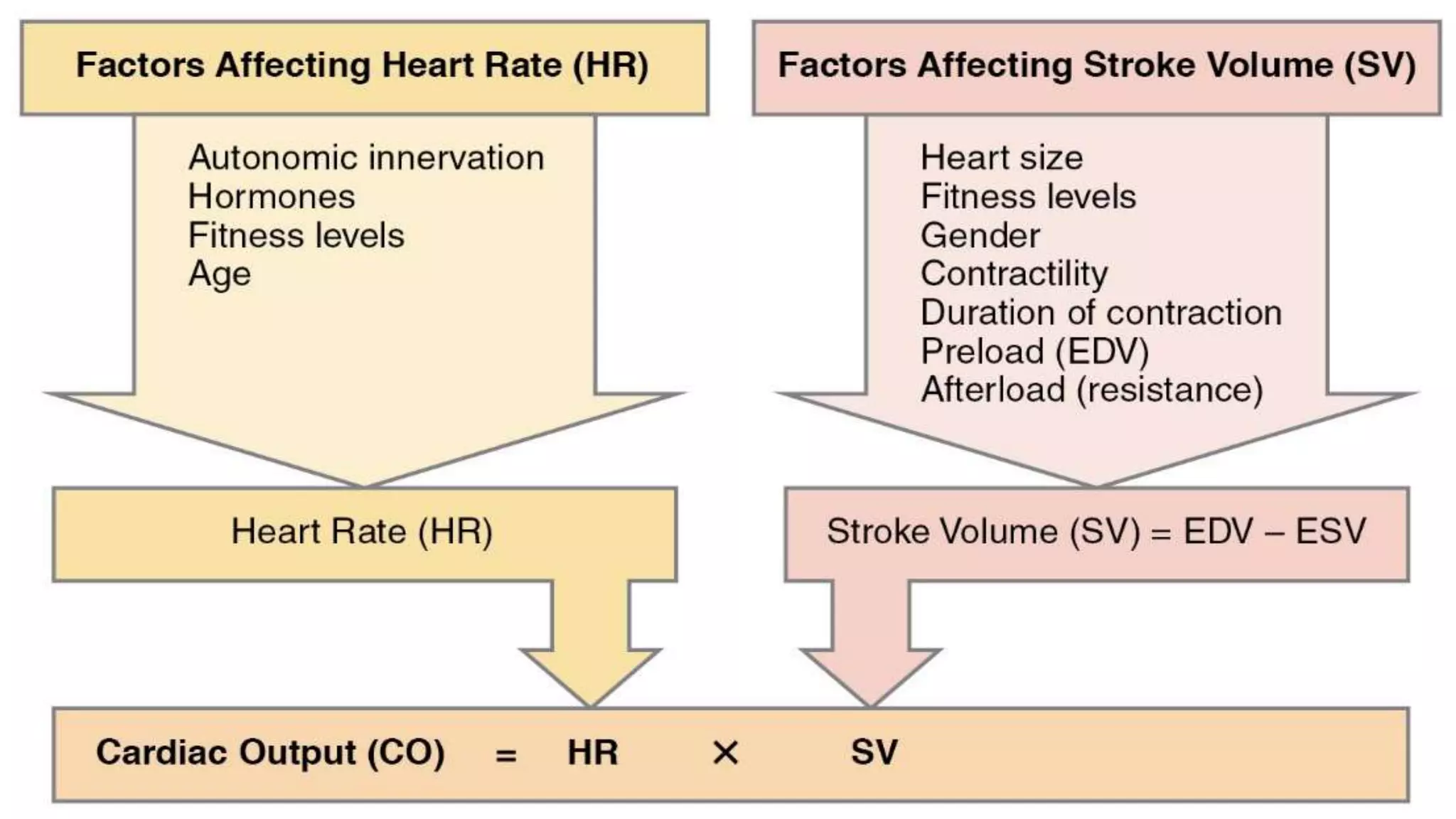
Cardiac output is the volume of blood pumped by the heart per minute and is equal to heart rate multiplied by stroke volume. Cardiac output can be expressed in three ways: stroke volume, minute volume, or cardiac index. Minute volume and cardiac output refer to the same thing in clinical practice. Stroke volume is the volume of blood pumped out of the left ventricle per contraction. Ejection fraction is the percentage of blood ejected from the ventricles during each contraction, normally 60-65%. Cardiac reserve is the maximum increase in cardiac output above normal levels, important for conditions like exercise.

































![CARDIO VASCULAR HEMODYNAMICSLab[1]](https://cdn.slidesharecdn.com/ss_thumbnails/cvm20lab1-1221330231981995-9-thumbnail.jpg?width=640&height=640&fit=bounds)


































