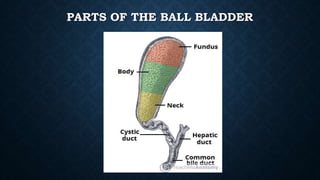
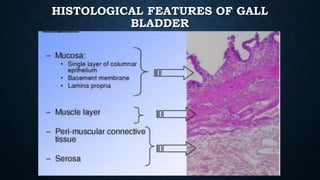
The document discusses carcinoma of the gallbladder, including its anatomy, types, stages, risk factors, symptoms, diagnostic findings, and management. The gallbladder stores and concentrates bile before digestion. Gallbladder carcinoma is often related to gallstones and is typically diagnosed via imaging and biopsy. Treatment involves surgery to remove the gallbladder and nearby tissues, and sometimes chemotherapy or radiation. Nursing care focuses on monitoring, diet, education on symptoms and lifestyle changes, and psychological support.