Downloaded 193 times
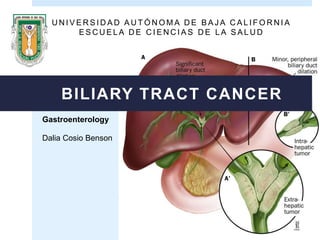
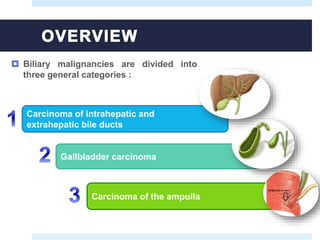
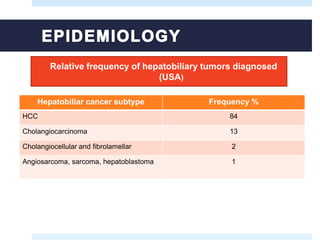
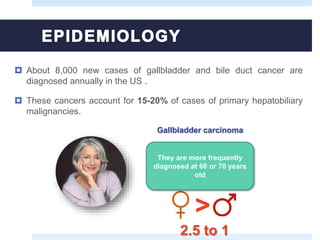
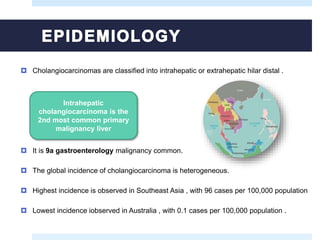
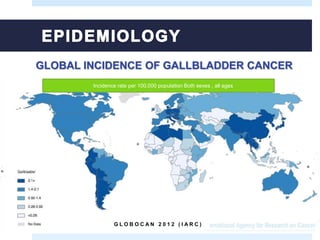
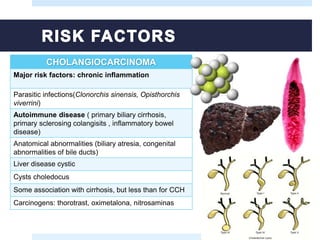
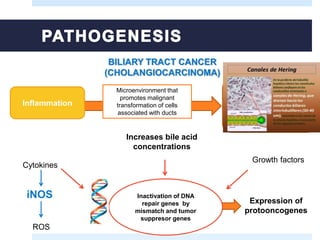
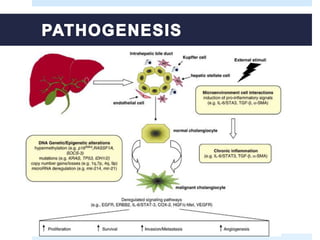
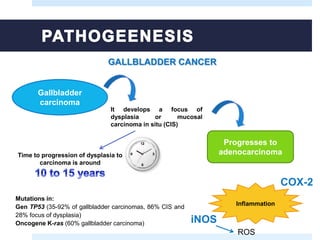
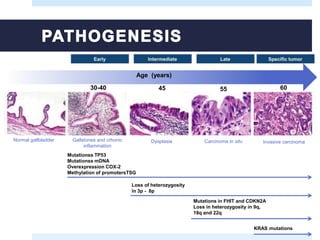
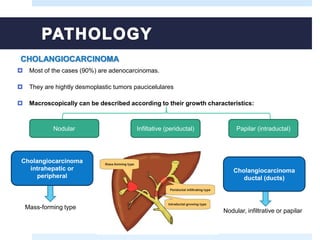
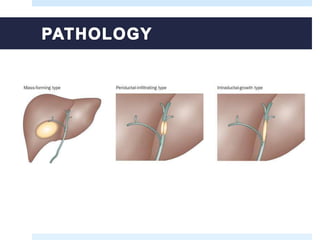
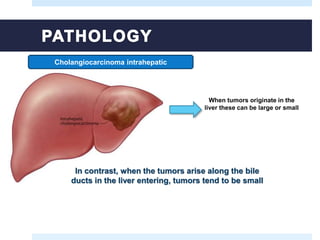
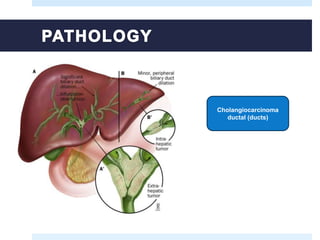
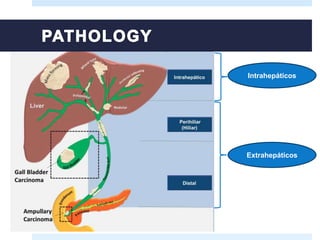
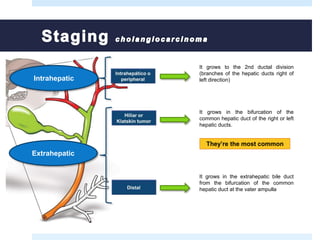
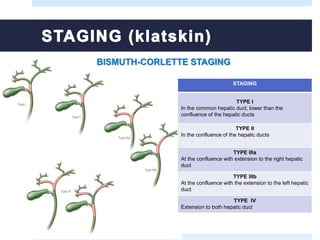
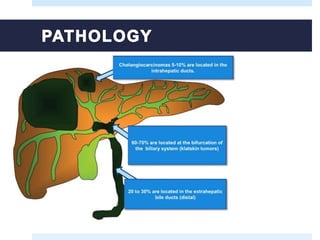
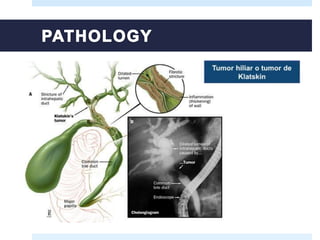
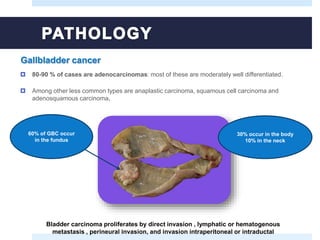
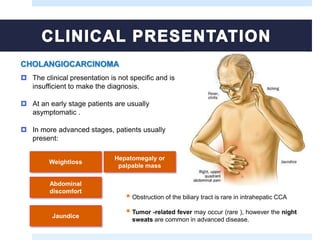
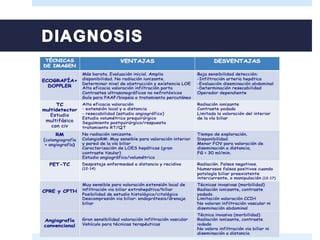
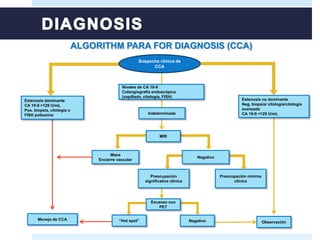
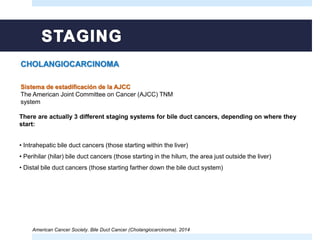
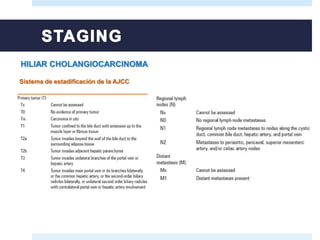
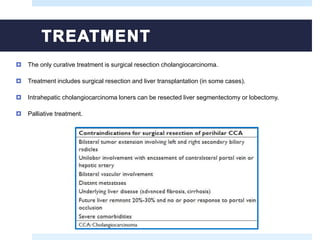
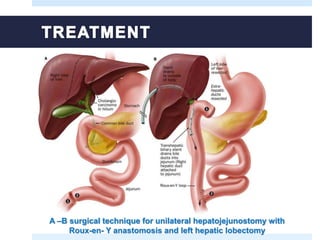
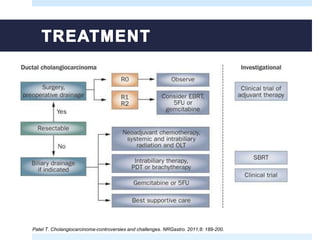
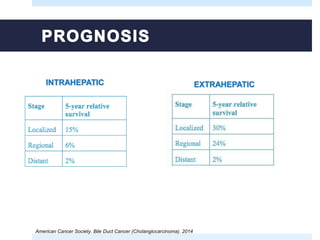
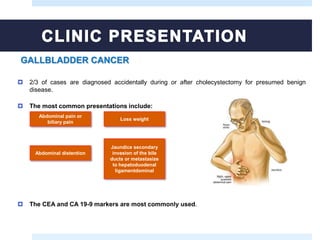
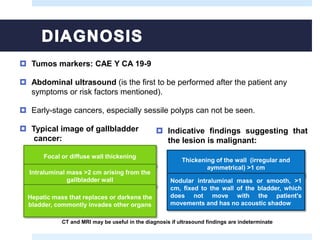
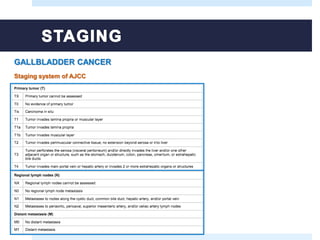
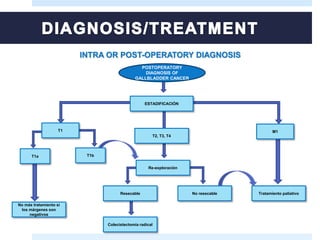

This document discusses biliary tract cancers including cholangiocarcinoma and gallbladder cancer. It provides information on risk factors, pathogenesis, clinical presentation, diagnostic evaluation, staging systems, and treatment options. Biliary tract cancers are generally diagnosed at late stages and have a poor prognosis. Surgical resection remains the only potentially curative treatment option, but palliative approaches are used for non-resectable disease.











































































