Downloaded 171 times

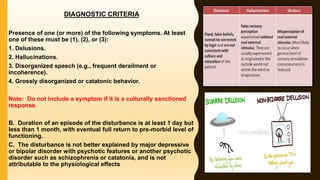


This document provides an overview of brief psychotic disorder according to diagnostic criteria in the DSM-V. It describes the disorder as a short duration severe mental disorder involving impaired thoughts and emotions where contact with reality is lost. The document outlines the diagnostic criteria including presence of delusions, hallucinations or other specified psychotic symptoms for at least one day but less than one month, followed by a full return to normal functioning. It also discusses associated features, risk factors, differential diagnoses, cultural considerations and prevalence.





















































































![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)

