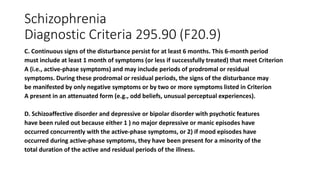
Schizophrenia spectrum and other psychotic disorders can involve abnormalities in delusions, hallucinations, disorganized thinking or speech, grossly abnormal motor behavior, and negative symptoms. Delusions are fixed false beliefs and can include persecutory, referential, grandiose, erotomanic, nihilistic, and somatic delusions. Hallucinations involve perceiving things without external stimuli and are most commonly auditory. Disorganized thinking involves loose associations, tangentiality, and incoherence. Grossly abnormal motor behavior includes catatonia which can involve negativism, stupor, and stereotyped movements. Brief psychotic disorder involves psychotic symptoms for less than 1 month while schizophren









































![Management
• Pharmacologic management traditional antipsychotics (dopamine- 2
[D2]-receptor antagonists) and atypical antipsychotic agents. Long-
acting injectable “depot” forms.
• Psychological management, including individual, family, and group
psychotherapy](https://image.slidesharecdn.com/psychoticdisorders-240224092543-3b95f3f8/85/psychotic-disorders-pptx-65-320.jpg)
















![schizophrenia_-final[1]psychiatry courses.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/schizophrenia-final1-241125165758-037ddbda-thumbnail.jpg?width=640&height=640&fit=bounds)
















































