Download to read offline




![How It Works??
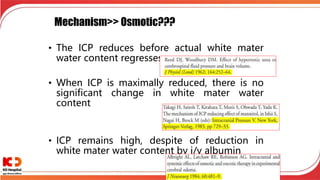
•Raising plasma osmolality from
310 mOsm/kgH2O to 344 mOsm/kgH2O can
shrink the brain by 10%, with half of the
shrinkage occurring in 12 minutes.
•Mannitol also reduces blood
viscosity [SURGICAL NEUROLOGY; Andrews,RJ;
39(3):218-222 (1993)] and oxidative damage.
•0.25-2 gm/kg body weight as 15-25%
solution
•Should be given fast over 20-30 minutes to
achieve peak effect](https://image.slidesharecdn.com/traumaticbraininjuryautosaved-230313134042-a66a1551/85/Traumatic-brain-injury-Autosaved-pptx-30-320.jpg)
![What is Ideal??
• Glycerol can be administered orally
• Long term Rebound edema
• >20% concentration Hemolysis
• BBB actively extrudes sodium, so less chance of
rebound edema with HS
• After initial dose (n=??) of mannitol causing brain
dehydration, repeated doses exacerbates edema
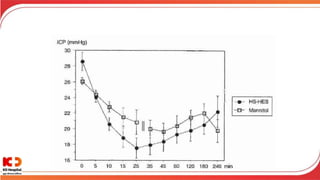
When given in an equimolar, rapid,
HSD reduces intracranial pressure more
than mannitol.
[Crit Care Med. 2005 Jan ;33:196-202; discussion
15644669]](https://image.slidesharecdn.com/traumaticbraininjuryautosaved-230313134042-a66a1551/85/Traumatic-brain-injury-Autosaved-pptx-33-320.jpg)




![Traumatic brain injury [Autosaved].pptx](https://image.slidesharecdn.com/traumaticbraininjuryautosaved-230313134042-a66a1551/85/Traumatic-brain-injury-Autosaved-pptx-65-320.jpg)

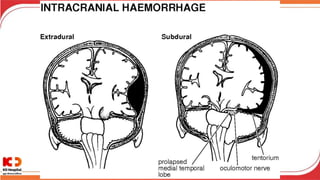
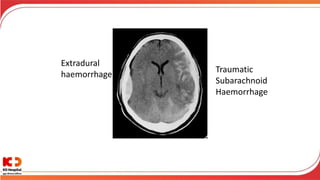
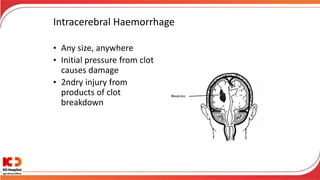
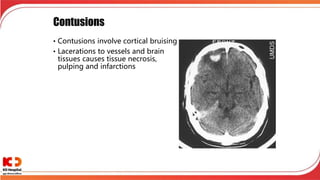
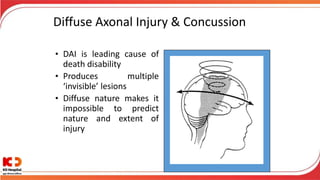
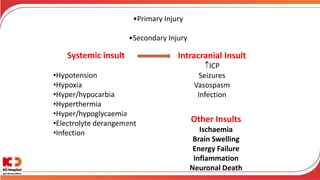
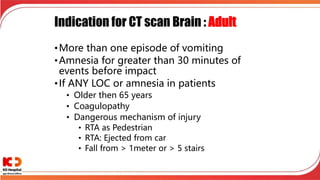
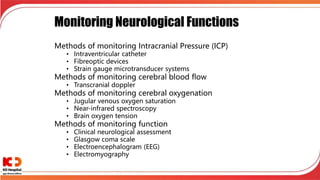
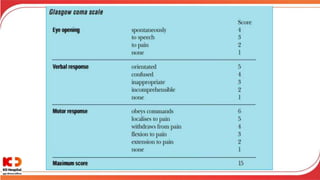
1. Traumatic brain injury can cause extradural haemorrhage, subarachnoid haemorrhage, intracerebral haemorrhage, contusions, and diffuse axonal injury from shearing and tearing of neurons. 2. Primary brain injuries occur at the time of impact while secondary injuries develop afterwards from processes like brain swelling and inflammation. 3. Brain injuries can be mild, moderate or severe depending on factors like loss of consciousness duration. Monitoring tools like ICP, CPP, oxygenation and imaging are important for management.




























![Balanced Crystalloids Webinar February 2023[2207].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/balancedcrystalloidswebinarfebruary20232207-240501141244-58dce968-thumbnail.jpg?width=640&height=640&fit=bounds)


























