Downloaded 102 times



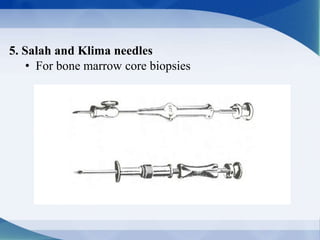
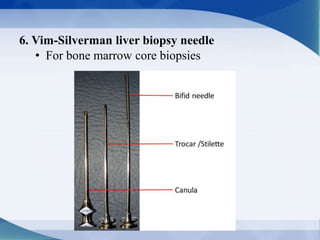

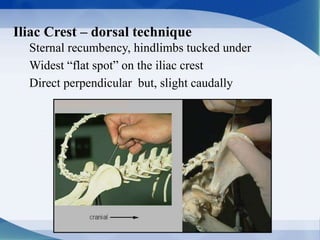

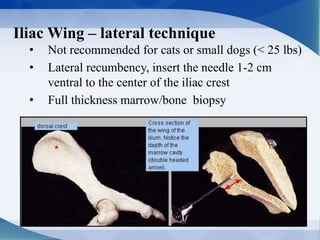
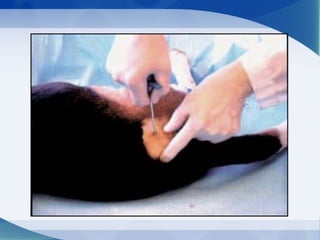
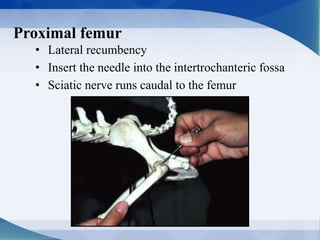

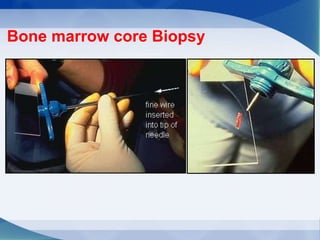
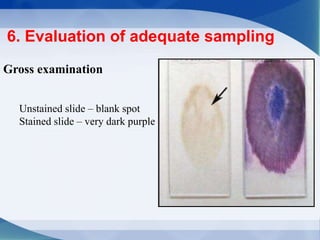
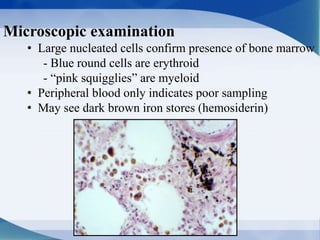


The document discusses bone marrow biopsy procedures. It describes: - Bone marrow as the flexible tissue within bone cavities that can be red (involved in blood cell production) or yellow (non-productive). - Indications for bone marrow biopsy including abnormal blood counts, infections, cancers, and iron storage investigations. - Precautions for biopsy in cases of bleeding disorders, anemia, or low platelet counts. - The steps of bone marrow biopsy including equipment, patient preparation, sample collection and evaluation, and sample submission.























































































