Downloaded 597 times

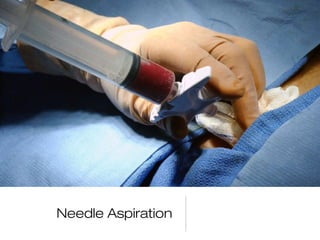
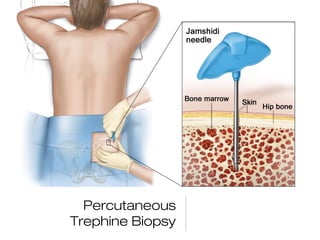

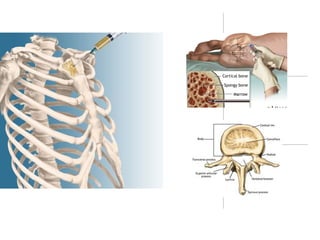

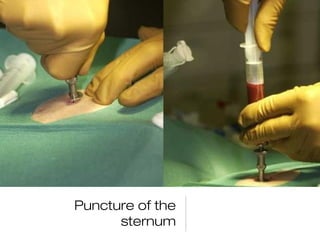


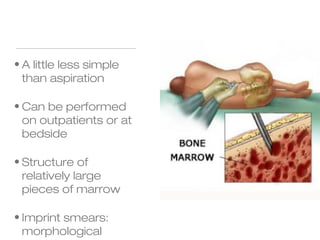
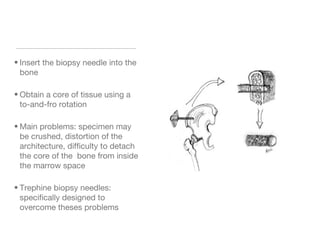
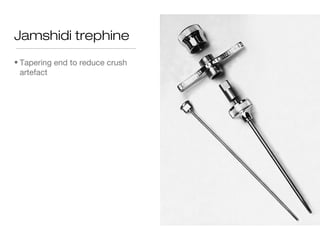

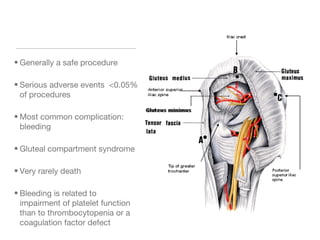
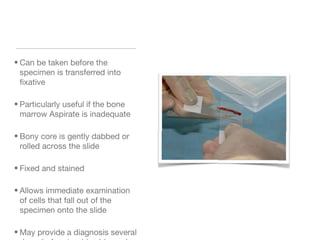

Bone marrow procedures involve bone marrow aspiration and trephine biopsy to examine the bone marrow. Bone marrow aspiration is a simple, safe outpatient procedure that allows examination of individual cells and their morphology. Trephine biopsy provides larger samples for examining marrow structure and architecture, and is valuable for diagnosing conditions with a "dry tap". Proper techniques and precautions are important to perform bone marrow procedures safely and obtain adequate samples for diagnosis.






























































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)




