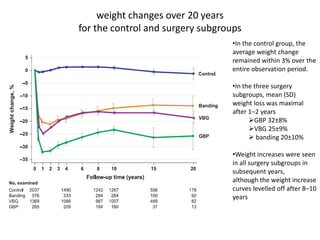
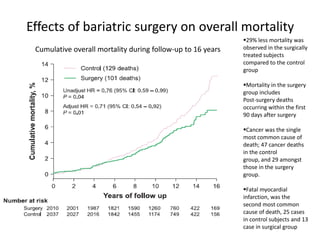
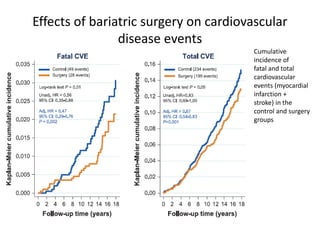
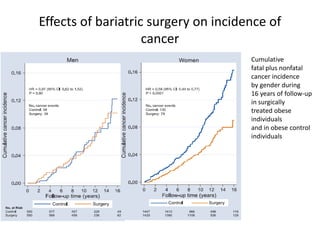
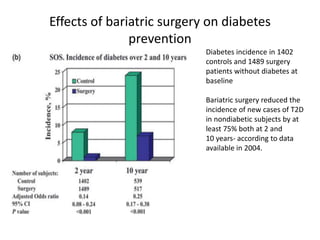
The Swedish Obese Subjects trial was a prospective study that compared outcomes of 2010 obese patients who underwent bariatric surgery to 2037 obese control patients who received conventional treatment. Over 20 years of follow up, bariatric surgery was associated with greater and longer-lasting weight loss compared to the control group. Bariatric surgery also reduced mortality by 29%, cardiovascular events by over 50%, diabetes incidence by at least 75%, and cancer incidence compared to conventional treatment alone. However, weight loss effects lessened over time, and some diabetes remission was not maintained after 10 years. The results provide evidence that bariatric surgery can improve health outcomes through weight loss, but weight-independent effects require further study.