1 CC: CaseI – Bleeding Disorder
Balance of hemostasis
- ระบบหามเลือดชา หรือ สลายลิ่มเลือดมากกวาปกติ -> Bleeding disorder
- ระบบหามเลือดทํางานมากกวาปกติ หรือ สลายลิ่มเลือดนอยกวาปกติ -> Arterial & Venous Thrombi
Mechanism of hemostasis
Hemostasis สวนที่เกี่ยวของ
Primary Platelet & Vessel
Secondary Clotting factors I-XIII
Tertiary
(Fibrinolytic system & Natural Anticoagulants)
Natural anticoagulant: Plasmin, Protein C, Protein S &
Anti-thrombin
Mechanism of Stop Bleeding
Hemostasis Mechanism
Primary เกิด Collagen (subendothelial) exposure (Endothelial injury)
1. Step: Activation/Secretion: Activated platelet ทําใหเกิด
o สราง: TXA2 -> Platelet aggregation (inhibit by NSIADs)
o สราง dense granule (ADP, Calcium, Histamine, Serotonin)
2. Step: Adhesion: Platelet จับกับโครงสรางอื่นดังนี้
o Collagen จับผาน GPIa-IIa receptor
o vonWillebrand จับผาน GP-Ib-IX-V
receptor
o Platelet ดวยกัน จับผาน GPIIb-IIIa
receptor และประสานกันดวย Fibrinogen
3. Step: Aggregation (อาศัย Coagulation cascade)
Secondary 1. In vitro cascade ใชในการอธิบาย PT, aPTT, TT เทานั้น ใชในการอธิบายโรคไมได
- Tenase complex = Factor VIIIa/IXa complex
- Prothrombinase complex = Factor Xa/Va complex
2.
2 CC: CaseI – Bleeding Disorder
2. In vivo cascade or waterfall cascade แบงออกเปน 3 phase
o Initiation: Tissue factor และ Factor VII เปลี่ยน IX -> IXa
(X –(IXa)-> Xa ; Prothrombin –(Xa)-> Thrombin)
o Amplification: Thrombin กระตุ9น Factor V,VIII,XI (XI กระตุน IX อีกที)
Activated platelet จะมี Va, VIIa, IXa อยูซึ่งสามารถกระตุน Factor อื่นได เชน
Factor IXa กระตุนใน Initation phase ได
o Propagation: Factor X -> Xa ดวย Tenase (Factor VIII, IX)
แลวทําใหเกิด “Thrombin Burst”
Note: Factor XIIIa เปน Fibrin stabilizing factor -> ทําใหเกิด fibrin cross-link (d-dimer)
Tertiary 1. Fibrinolytic pathway
- Free plasmin จะถูก neutralized by α2-antiplasmin ที่สรางจากตับ*
o ในคนไข cirrhosis อาจพบฺ Bleeding disorder - Hyperfibrinolysis ได
จาก α2-antiplasmin deficiency ทําใหPlasmin เยอะ
* ผลแลปที่สําคัญ คือ D-dimer จะไมพบวาสูง เพราะ Factor XIII ทํางานไมทันการ
ทํางานของ plasmin ที่ทํางานเร็วเหลือเกิน
- Pathway ที่สามารถกระตุน plasminogen -> plasmin ไดนั้น มี 4 pathway ไดแก
o Plasminogen activator (t-PA & u-PA)
o Kinase pathway (Streptokinase)
o Contact factor pathway (In vivo: Factor XII, Kallikrein, Prekallikrein)
o Exogenous pathway (recombinant t-PA)
- Fibrin ภายหลังจะถูกเปลี่ยนเปน Fibrin degradation product (D-dimer) – ใชเปน Lab
indication of deep vein thrombosis / pulmonary embolism
- Fibrinogen (มี α,β chain) ที่จะเปลี่ยนเปน Fibrin polymer ได ตองถูก cleave เปน
Fibrinopeptide A และ Fibrinopeptide B หากตัดแคอยางใดอยางหนึ่ง จะรวมเปน polymer
ไมได และจะถูก plasmin สลายกลายเปน Fibrin degradation product
- Factor XIII deficiency:
o จะไมสามารถรวมเปน Fibrin polymer ไดสมบูรณq (ขาดการสราง D-dimer) จึงไม
สามารถสลายเปน degradation product ได
o aPTT & PT normal เพราะวาในหองปฏิบัติการสิ้นสุดแคการสราง fibrin monomer
3.
3 CC: CaseI – Bleeding Disorder
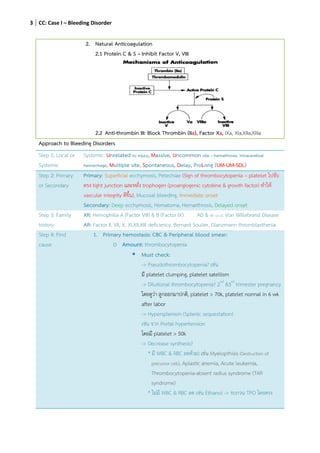
2. Natural Anticoagulation
2.1 Protein C & S – Inhibit Factor V, VIII
2.2 Anti-thrombin III: Block Thrombin (IIa), Factor Xa, IXa, XIa,XIIa,XIIIa
Approach to Bleeding Disorders
Step 1: Local or
Systemic
Systemic: Unrelated to injury, Massive, Uncommon site – hemathrosis, intracerebral
hemorrhage, Multiple site, Spontaneous, Delay, ProLong (UM-UM-SDL)
Step 2: Primary
or Secondary
Primary: Superficial ecchymosis, Petechiae (Sign of thrombocytopenia – platelet ไปจับ
ตรง tight junction และหลั่ง trophogen (proangiogenic cytokine & growth factor) ทําให
vascular integrity ดีขึ้น), Mucosal bleeding, Immediate onset
Secondary: Deep ecchymosis, Hematoma, Hemarthrosis, Delayed onset
Step 3: Family
history
XR: Hemophilia A (Factor VIII) & B (Factor IX) AD & AR (2n,3): Von Willebrand Disease
AR: Factor II, VII, X, XI,XII,XIII deficiency, Bernard Soulier, Glanzmann thromblasthenia
Step 4: Find
cause
1. Primary hemostasis: CBC & Peripheral blood smear:
o Amount: thrombocytopenia
Must check:
-> Pseudothrombocytopenia? เชน
มี platelet clumping, platelet satellism
-> Dilutional thrombocytopenia? 2nd
&3rd
trimester pregnancy
โดยดูวา ลูกออกมาปกติ, platelet > 70k, platelet normal in 6 wk
after labor
-> Hypersplenism (Splenic sequestation)
เชน จาก Portal hypertension
โดยมี platelet > 50k
-> Decrease synthesis?
* มี WBC & RBC ลดดวย) เชน Myelopthisis (Destruction of
precursor cell), Aplastic anemia, Acute leukemia,
Thrombocytopenia-absent radius syndrome (TAR
syndrome)
* ไมมี WBC & RBC ลด เชน Ethanol -> รบกวน TPO โดยตรง
4.
4 CC: CaseI – Bleeding Disorder
-> Increase destruction
เชน Immune Thrombocytopenia (ITP), Microangiopathic
Hemolytic Anemia (MAHA)
o Function: Abnormal bleeding time & platelet aggregation test
Must check:
-> Acquired Platelet Dysfunction
a. Uremia ดู BUN, Cr (รบกวนการสราง TXA2)
b. Drugs เชน NSAIDs, Calcium blocker
c. Myeloproliferative disease เชน Polycythemia vera (WBC,
RBC, Platelet เพิ่มแตไมมีประสิทธิภาพ)
d. Paraproteinemia เปนภาวะที่มีโปรตีนบางชนิดในเลือดสูงรบกวน
การทํางานของเกล็ดเลือดเชนโรค multiple myeloma
e. Myelodysplastic syndrome – Ineffective production
f. Acquired platelet function with eosinophilia (APDE)
-> Congenital Platelet Dysfunction
a. Bernard-Soulier syndrome
b. Von Willebrand disease
c. Glanzmann thrombasthenia
d. Storage pool disease – lack
of dense granule
2. Secondary hemostasis: PT & aPTT & TT
How to find cause of Secondary hemostatic defect
PT aPTT TT Disease
N N N Mild bleeding disorder เชน mild vWD,
Factor XIII deficiency,
Hyperfibrinolysis,
Vascular disease (Ehler Danlos syndrome – Collagen synthesis defect,
Osler Weber Rendu syndrome – Angiogenesis defect, Marfan syndrome, Scurvy)
P N N Factor VII deficiency or inhibitor (Extrinsic pathway), Early liver impairment* Factor VII ไป
กอนเพราะ half-life สั้นที่สุด, DIC
Vitamin K deficiency (กระทบ Factor II, VII, IX, X) or Vitamin K antagonist
N P N มีเลือดออกผิดปกติ:
Factor VIII, IX, XI deficiency or inhibitor
VonWillebrand disease (vWF carries Factor VIII)
ไมมีเลือดออกผิดปกติ: Factor XII, HMWK or Prekallekrein deficiency or inhibitor
Lupus anticoagulant (Antiphospholipid syndrome – hypercoagulable state)
P P N Liver Impairment, Vitamin K deficiency or antagonist (ผลตอ Factor II, VII, IX, X)
5.
5 CC: CaseI – Bleeding Disorder
Factor II, V, X deficiency or inhibitor, Massive transfusion
P P P Heparin contamination (IIa, Xa) – Repeat test โดยใช Batroxobin แทน thrombin (เพราะไม
ถูกยับยั้งดวย Heparin-ATIII complex), Overt DIC, Monoclonal gammopathy
(Paraproteinemia)
Factor I: Afibrinogenemia, Hypofibrinogenemia, Dysfibrinogenemia
Note: Deficiency กับ inhibitor แยกกันดวย Mixing test โดยเอาเลือดปกติ ผสมกับเลือดผิดปกติ ถา Deficiency พอเติม
เลือดปกติ Lab value จะกลับมา normal
จากนั้นอาจทํา Factor assay เพื่อการวินิจฉันโรคอยางจําเพาะตอไป
Medication
Antithrombotic Drugs – อJานเพิ่มจากแหลJงอื่น
Anticoagulants
1. Heparin – Cofactor of Anti-thrombin III:
o Unfractionated Heparin (UFH) blocks factor IIa, Xa
ตองดู aPTT* – ตองดูใหได 2-2.5 เทาจากคาปกติ
o LMW or Fondaparinux blocks factor Xa
ไมตองวัด aPTT แตใหดูตามน้ําหนักตัวผูป~วย
ในกรณีผูป~วยไตวาย ตองวัด anti-factor Xa activity
Use: ป•องกันและรักษา thromboembolic disease เชน Deep vein thrombosis, Pulmonary embolism
(ออกฤทธิ์เร็วกวา Warfarin เพราะยับยั้งเลย ไมไดรบกวนการสราง)
2. Warfarin – Inhibit epoxide reductase (ใช activate Vitamin K ซึ่งจําเปนตอ γ − ในการสราง
factor II, VII, IX, X)
ตองดู PT* ซึ่งจะเห็นผลชัดเมื่อ Factor ลดลงประมาณ 10-40%
ผลโดยออม เมื่อ Factor II จะมีผลลดการทํางานของ Protein C & S ดวย เพราะจะมี
Thrombin ลดลง
Use: ป•องกันและรักษา thromboembolic disease เชน Deep vein thrombosis, Pulmonary embolism
(ตามหลังการให heparin)
ป•องกัน Thromboembolism in prostatic heart valve & chronic atrial fibrillation