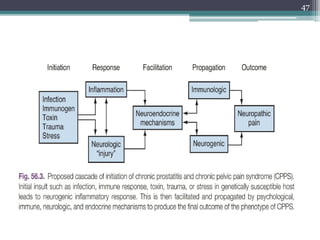
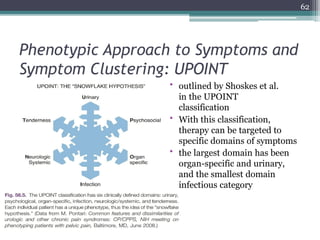
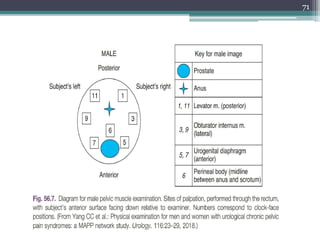
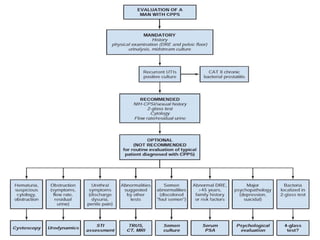
The document discusses chronic pelvic pain syndrome, focusing on prostatitis, its classification, historical context, and diagnostic criteria established by the NIH. It details various types of prostatitis, including acute bacterial and chronic bacterial prostatitis, their symptoms, treatments, and associated risk factors while highlighting the complexities of chronic pelvic pain and its multifactorial etiology. It further examines the histopathological features, immunological factors, and psychosocial influences impacting patients with chronic prostatitis and pelvic pain.