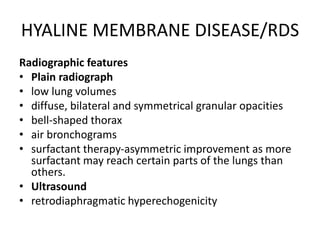
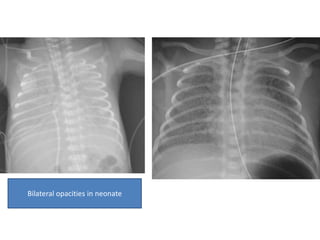
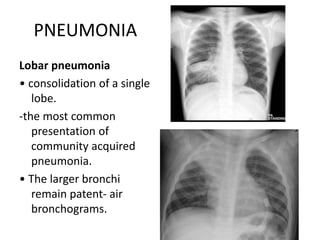
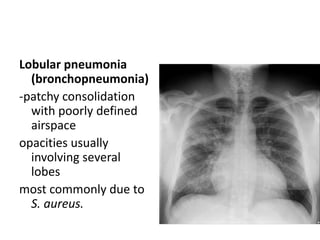
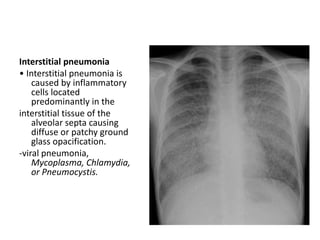
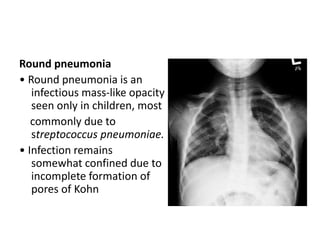
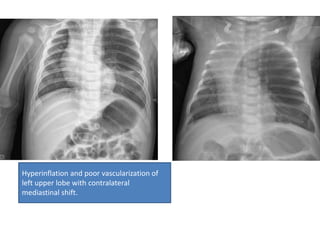
This document discusses several pediatric lung conditions seen on radiography including hyaline membrane disease, pneumonia, collapse, and congenital lobar emphysema. Hyaline membrane disease presents with low lung volumes, diffuse granular opacities, and air bronchograms. Pneumonia can appear as lobar consolidation, lobular patchy opacities, interstitial ground glass infiltrates, or rounded masses. Collapse is identified by volume loss, fissure displacement, and mediastinal shift. Congenital lobar emphysema involves overinflation of one lobe with oligemia and mediastinal shift.