
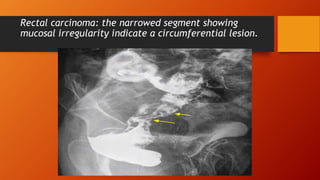
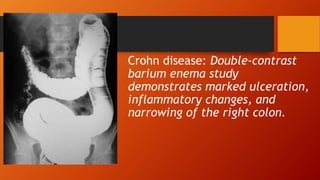

A barium enema is a radiographic procedure used to examine the large intestine. During the procedure, a liquid suspension of barium sulfate is introduced into the rectum to coat the intestinal walls. X-rays are then taken to visualize the colon. It allows visualization of the entire colon and can detect conditions like colon cancer, inflammatory bowel disease, and diverticulitis. Proper preparation and positioning of the patient is important. Double contrast technique involves injecting air in addition to barium to better visualize the mucosal lining. Findings are evaluated for abnormalities that may indicate diseases of the colon.
![COMPLETE BARIUM STUDIES Of GIT NAD [Adrian Dungu Niyimpa].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/bastudies-gitnad-220902221043-d535eaa3-thumbnail.jpg?width=640&height=640&fit=bounds)


































































