Download to read offline










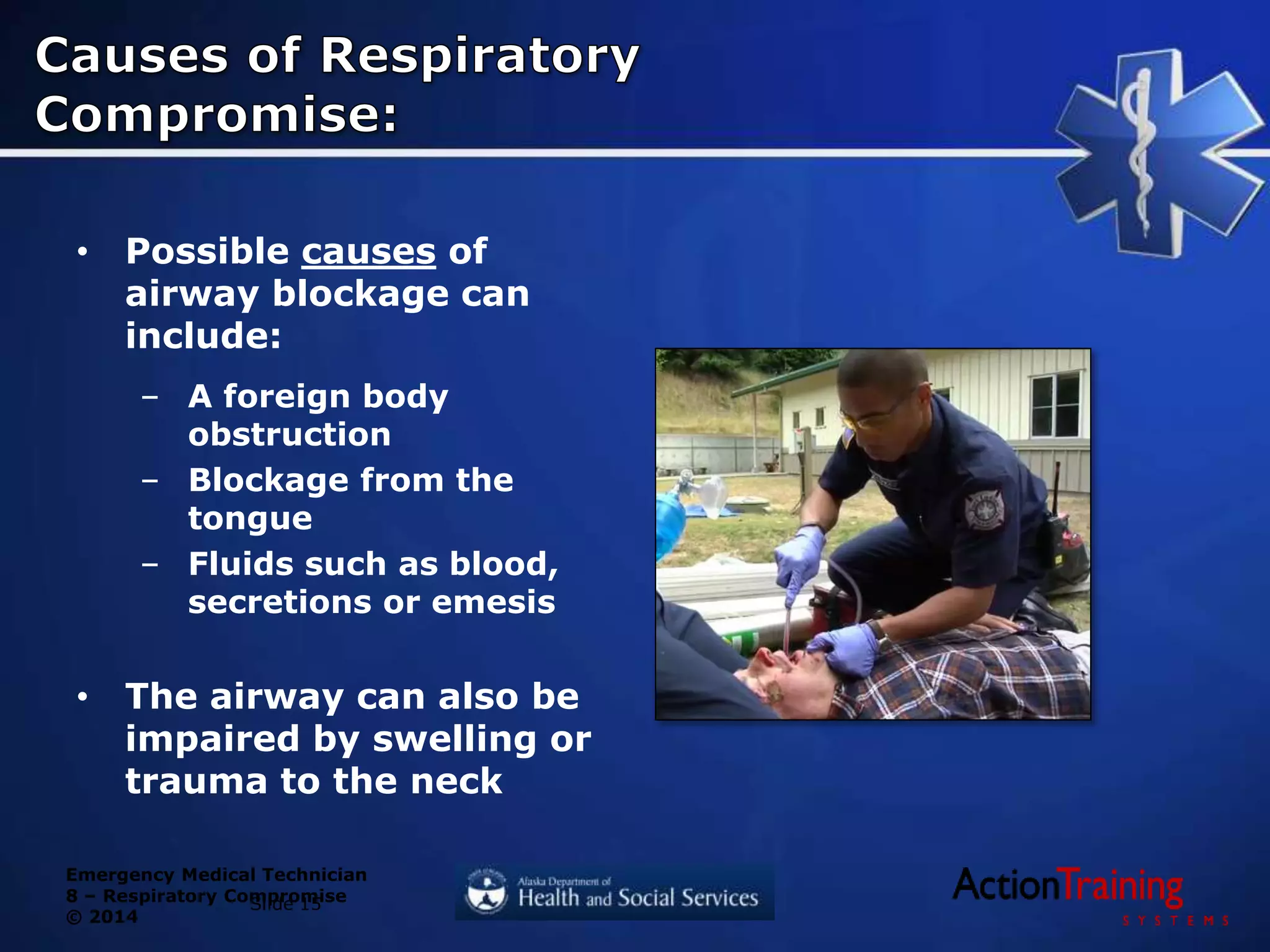


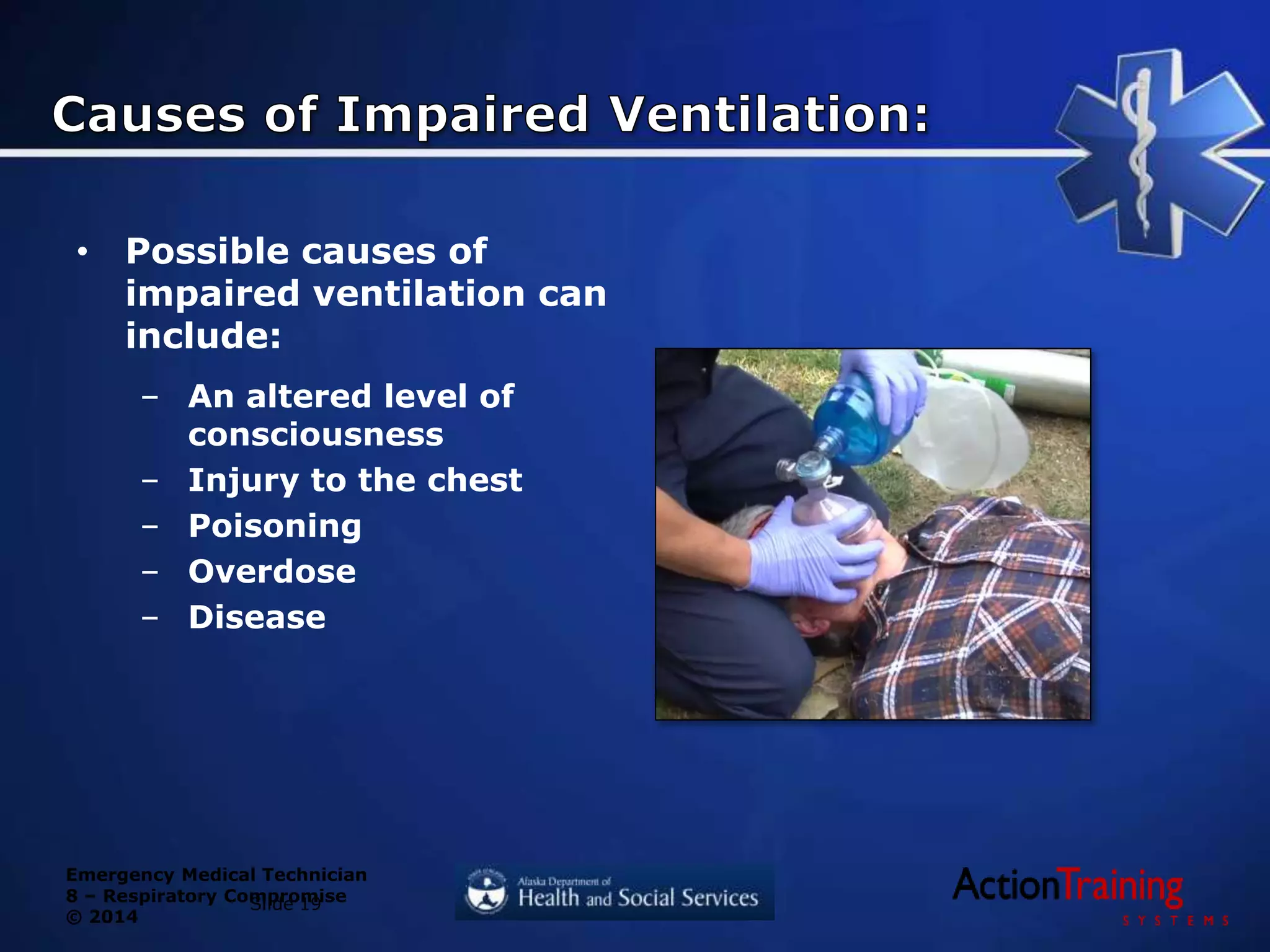
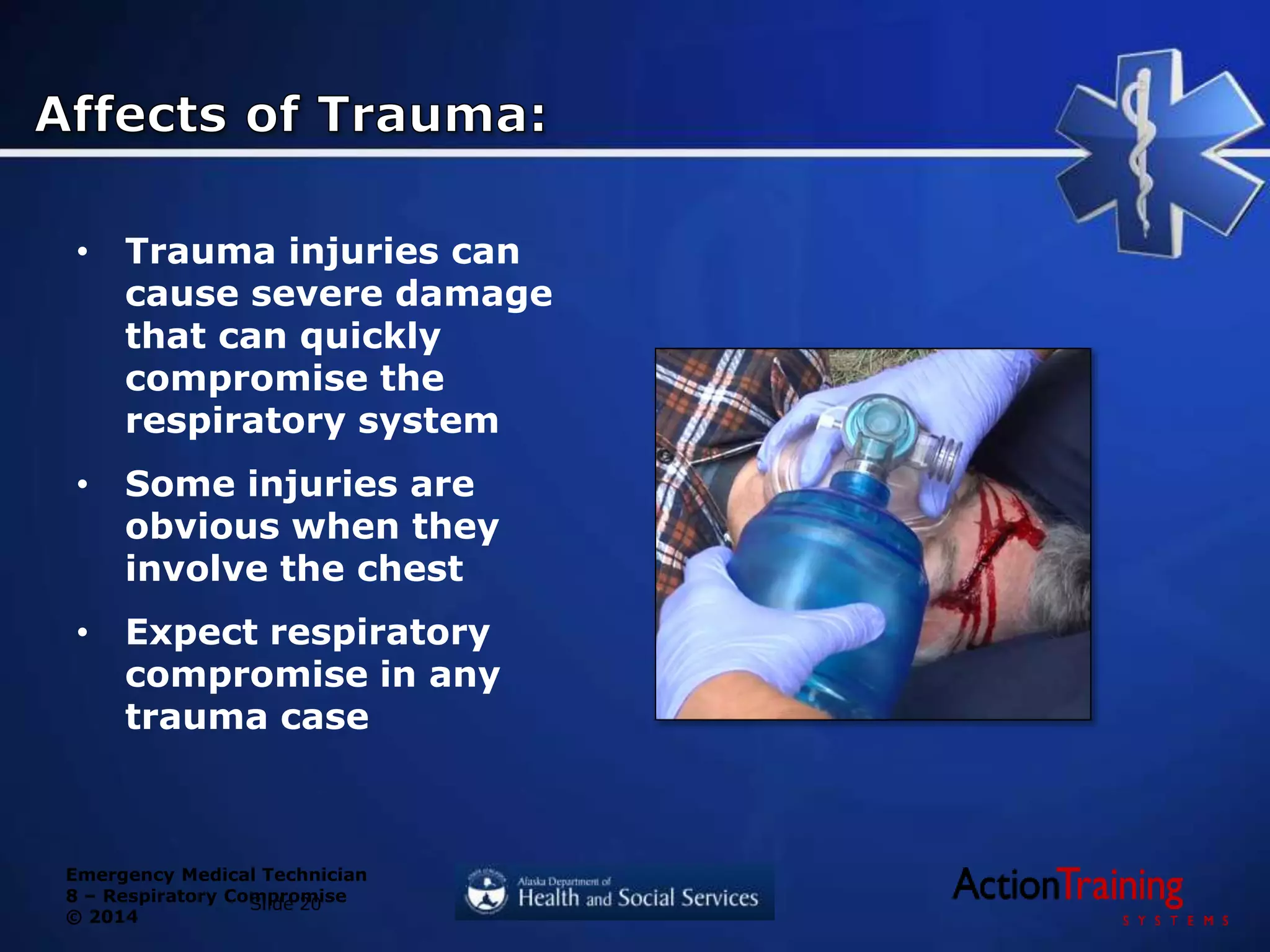











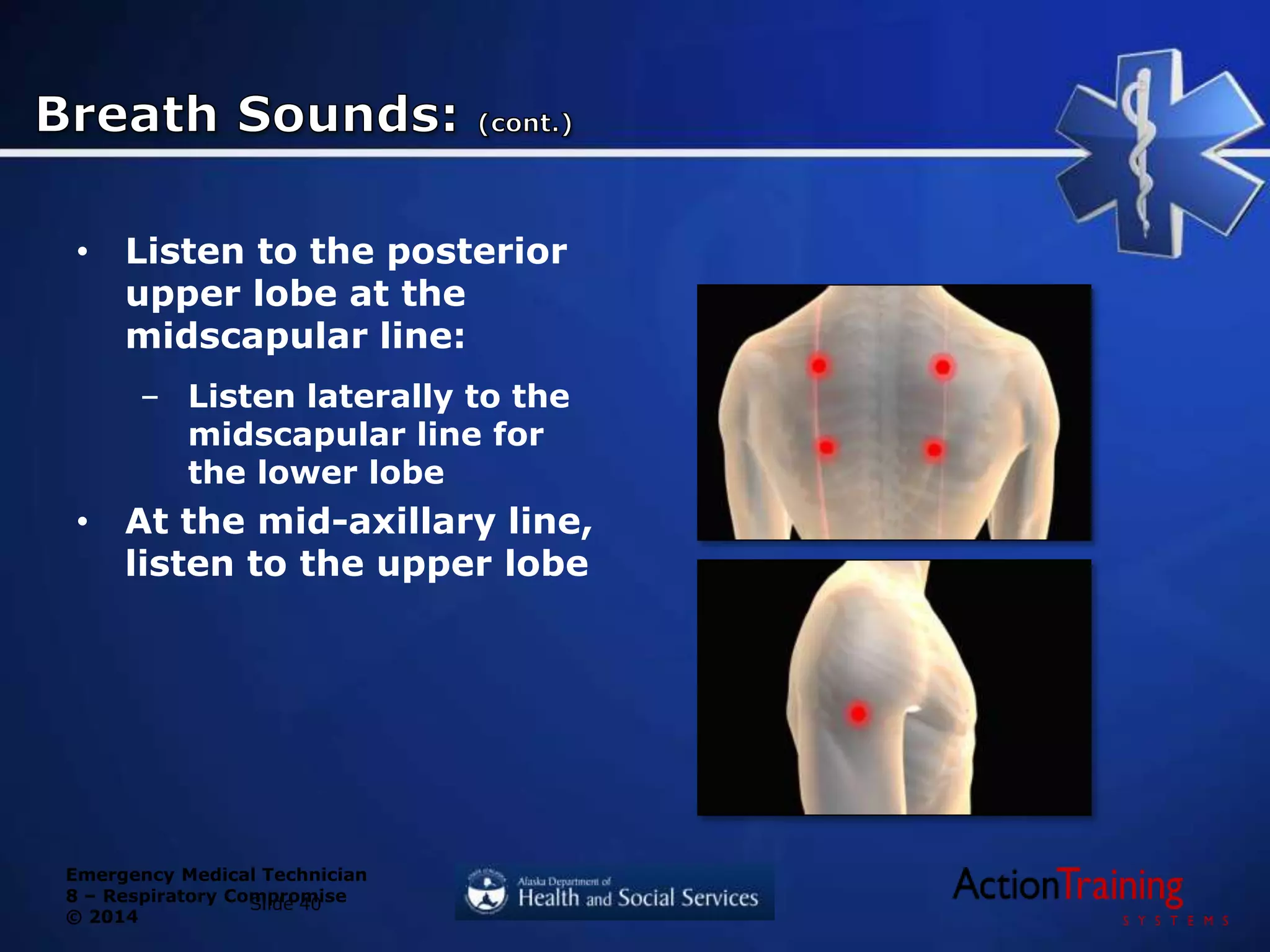




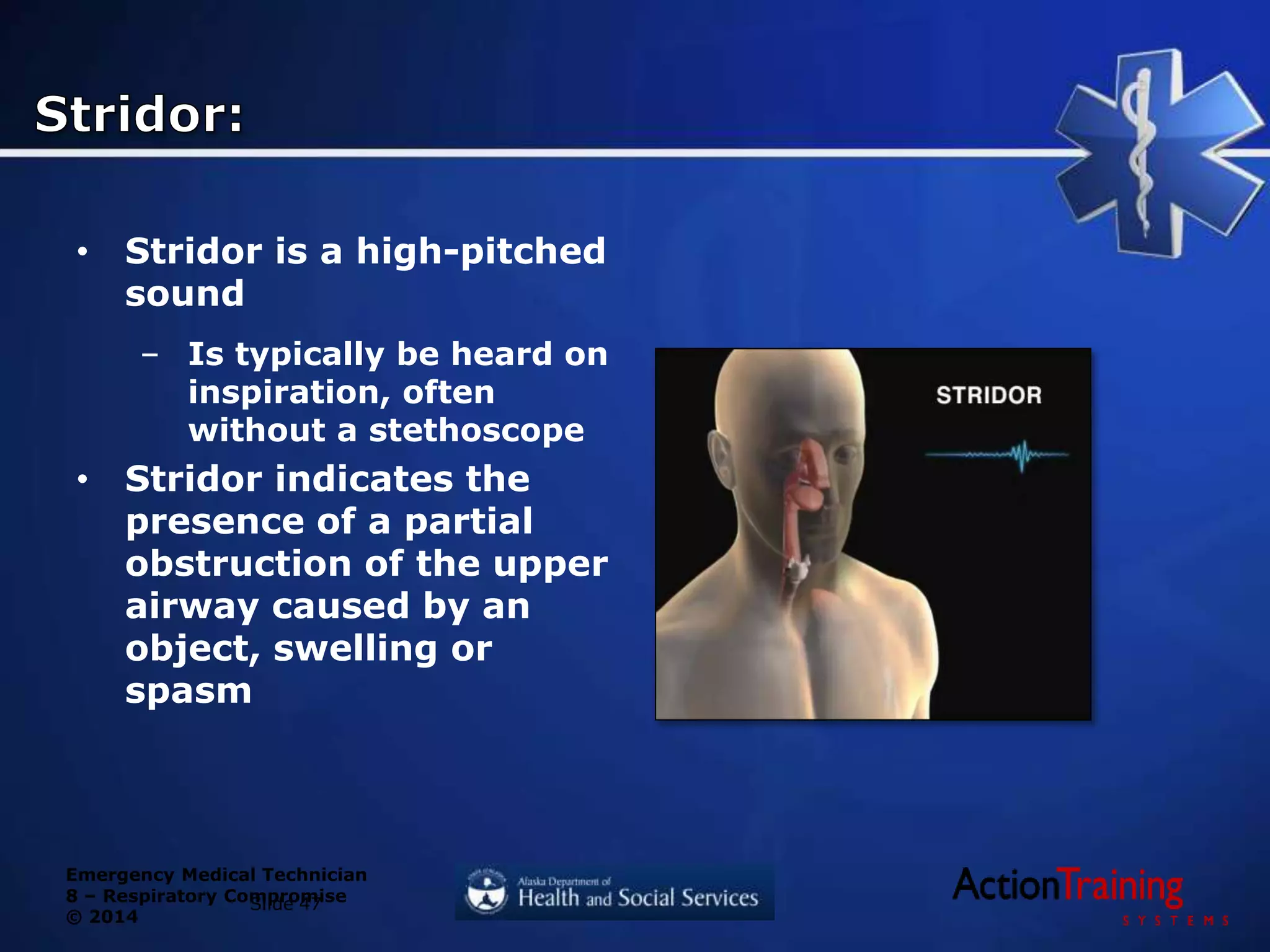

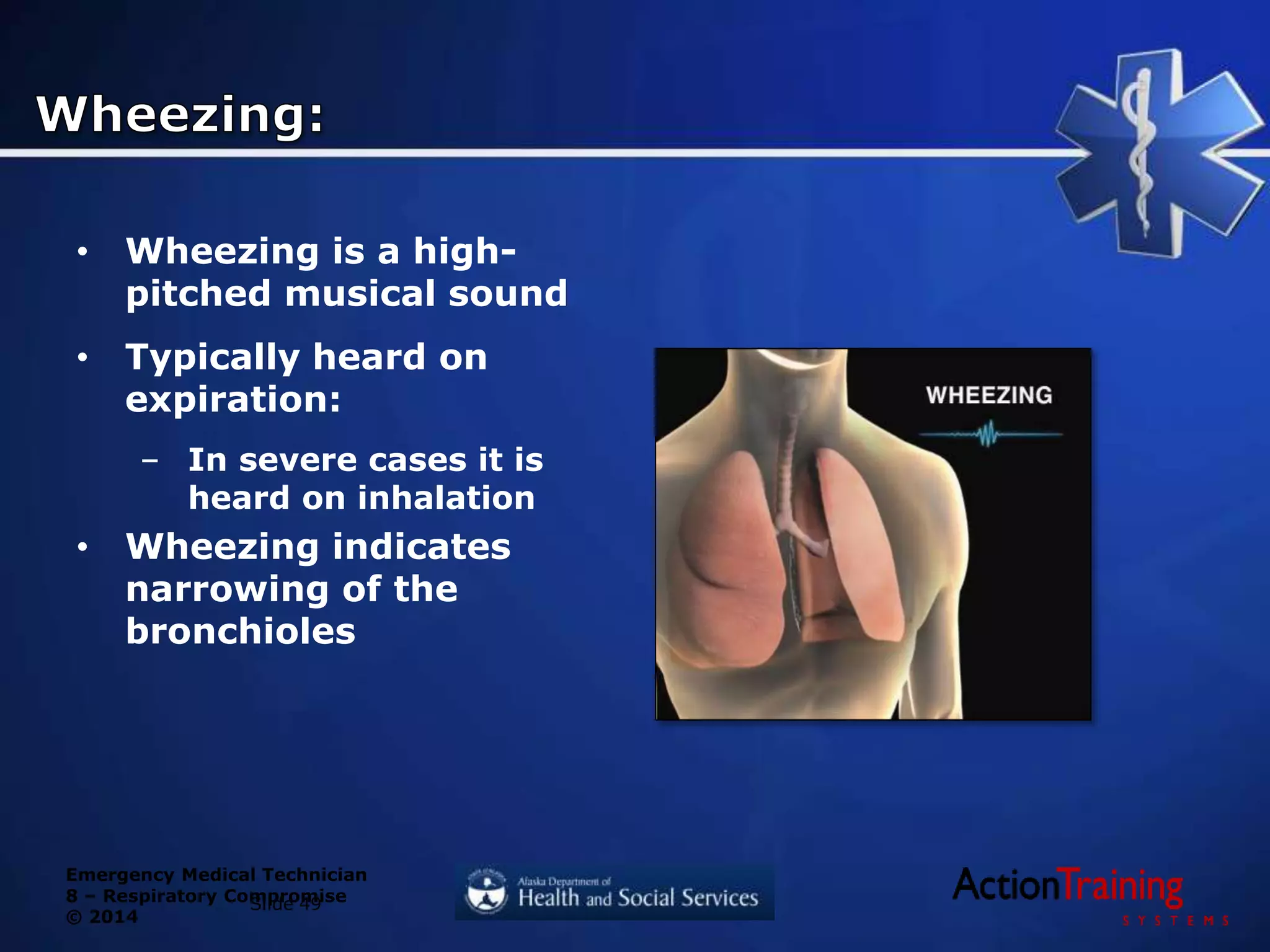
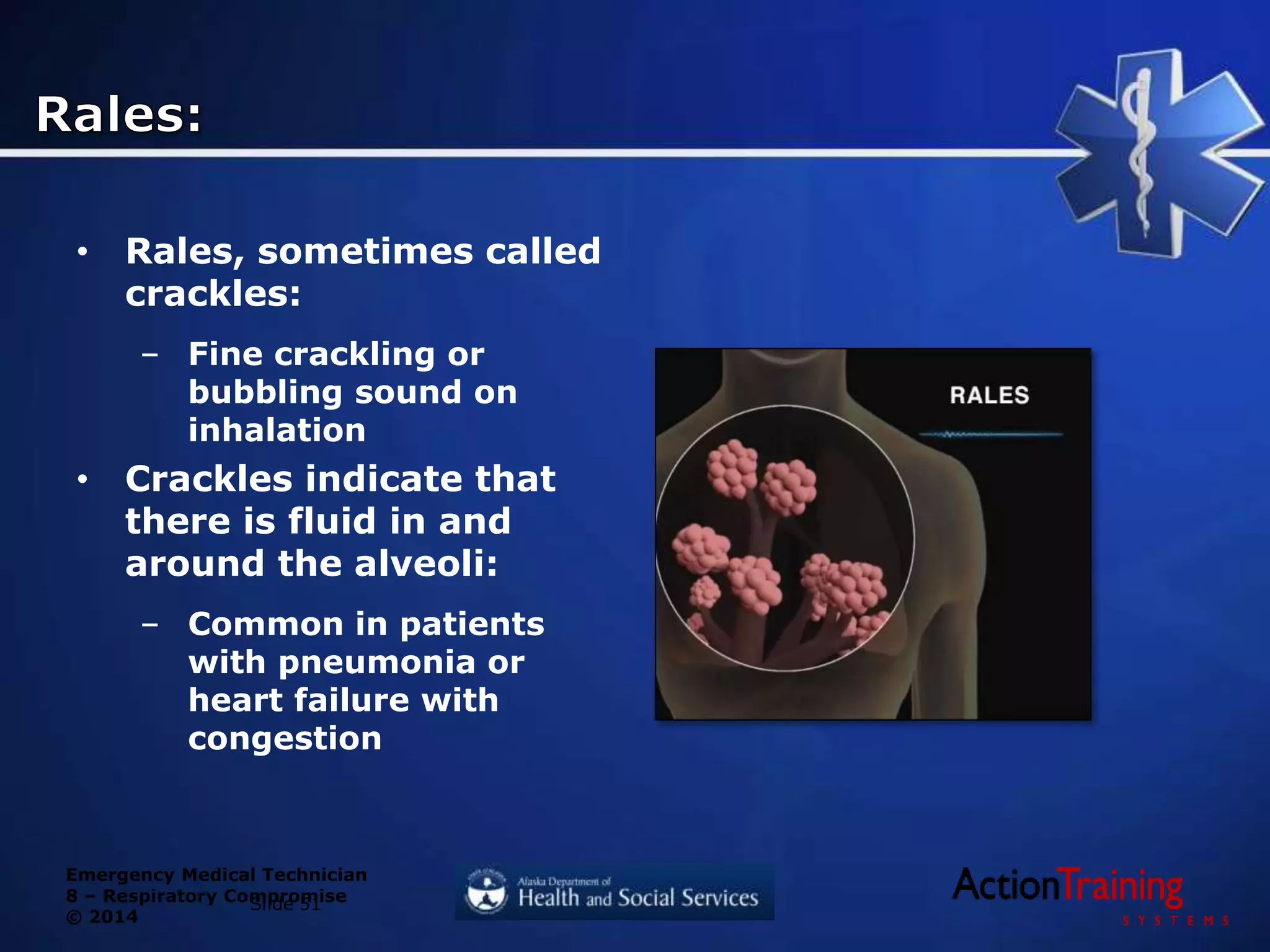










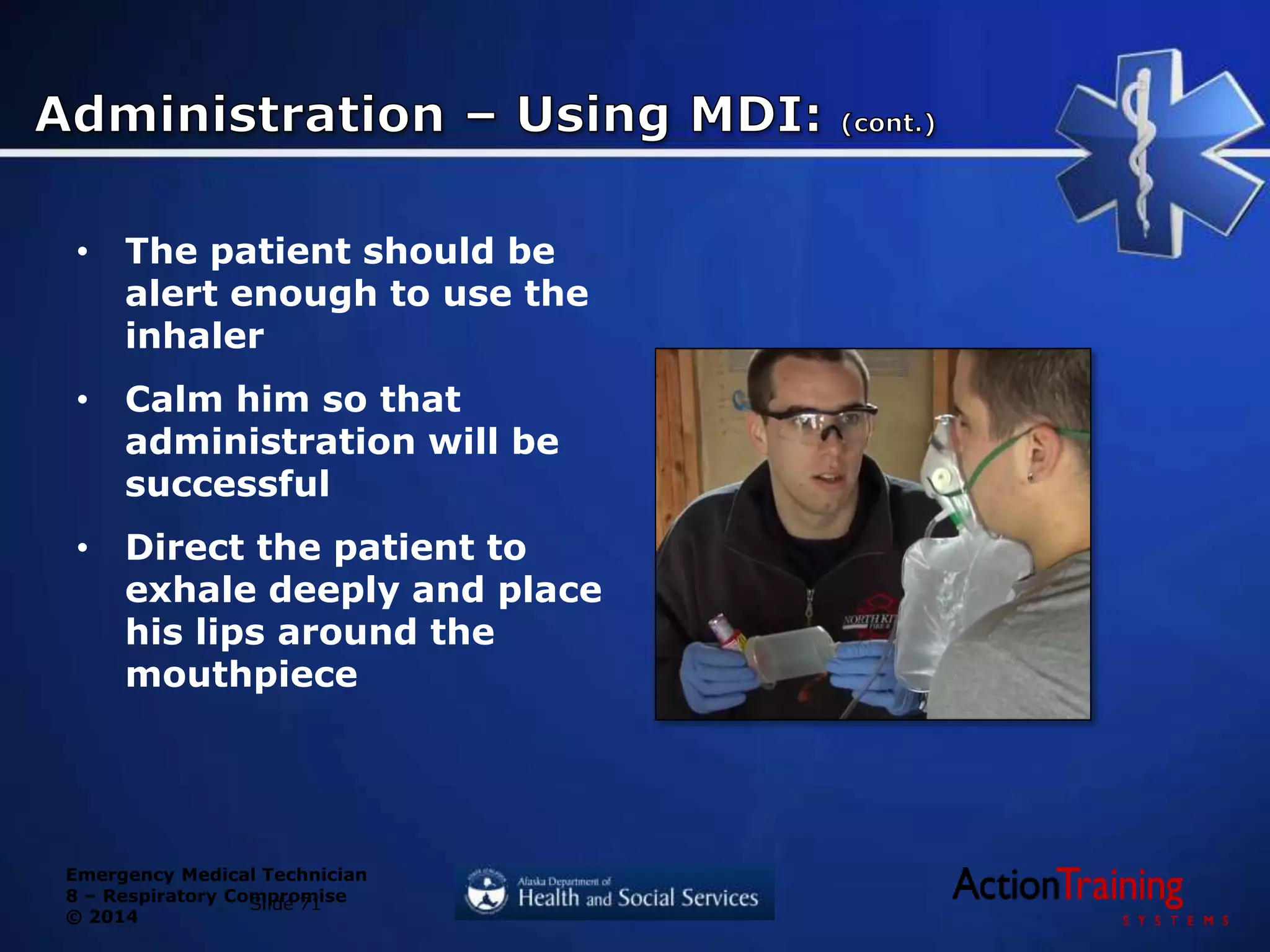

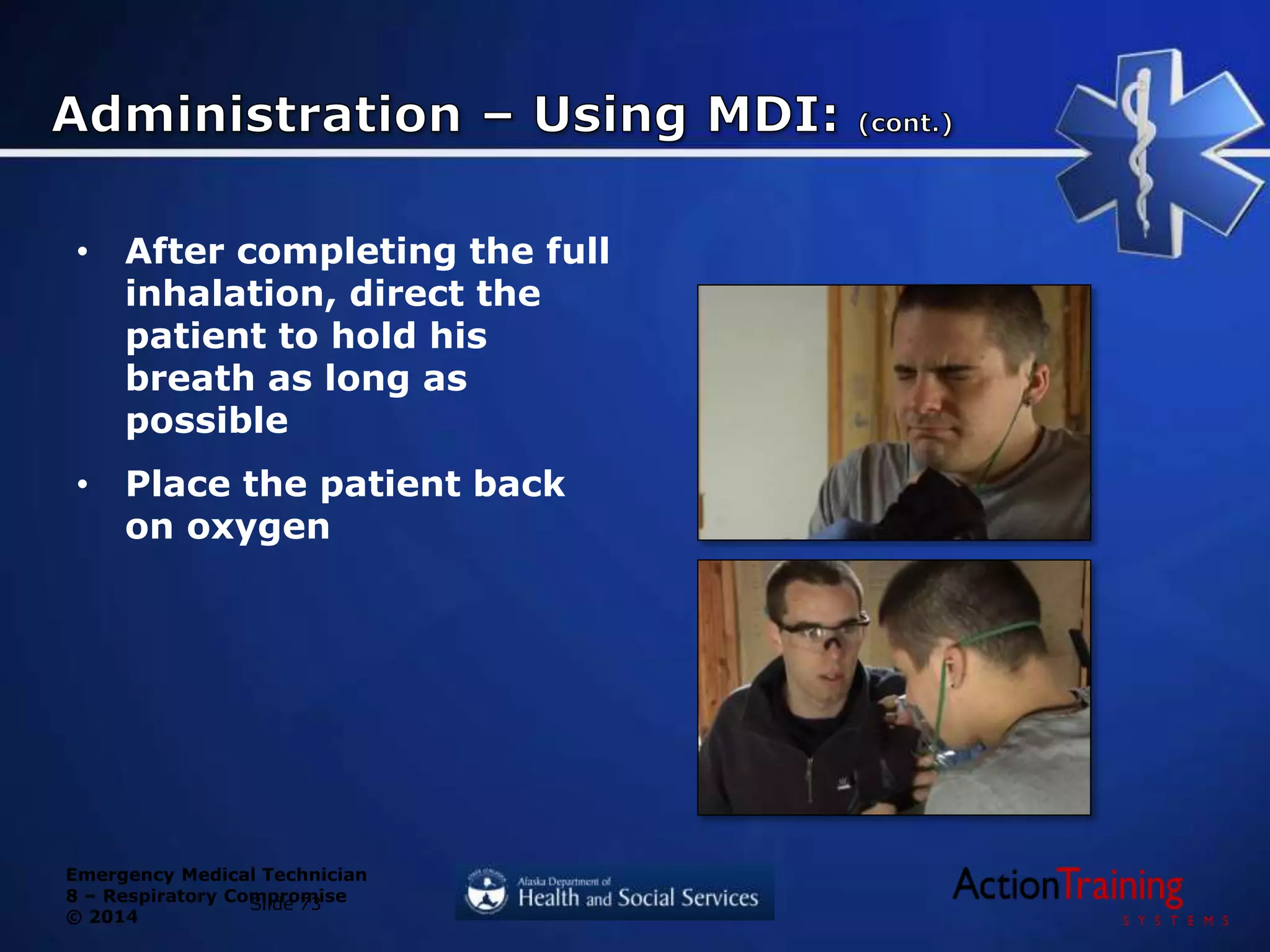


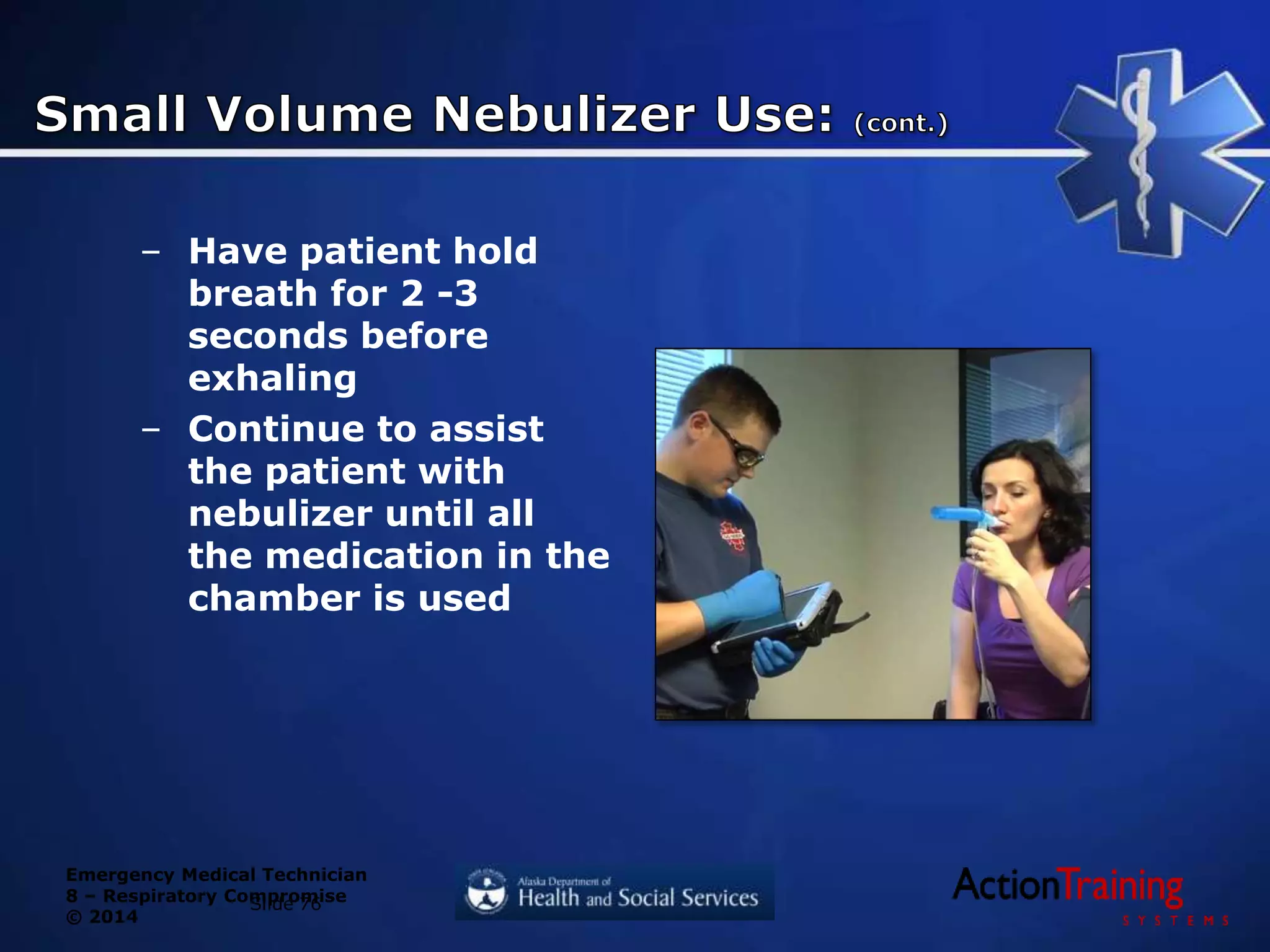

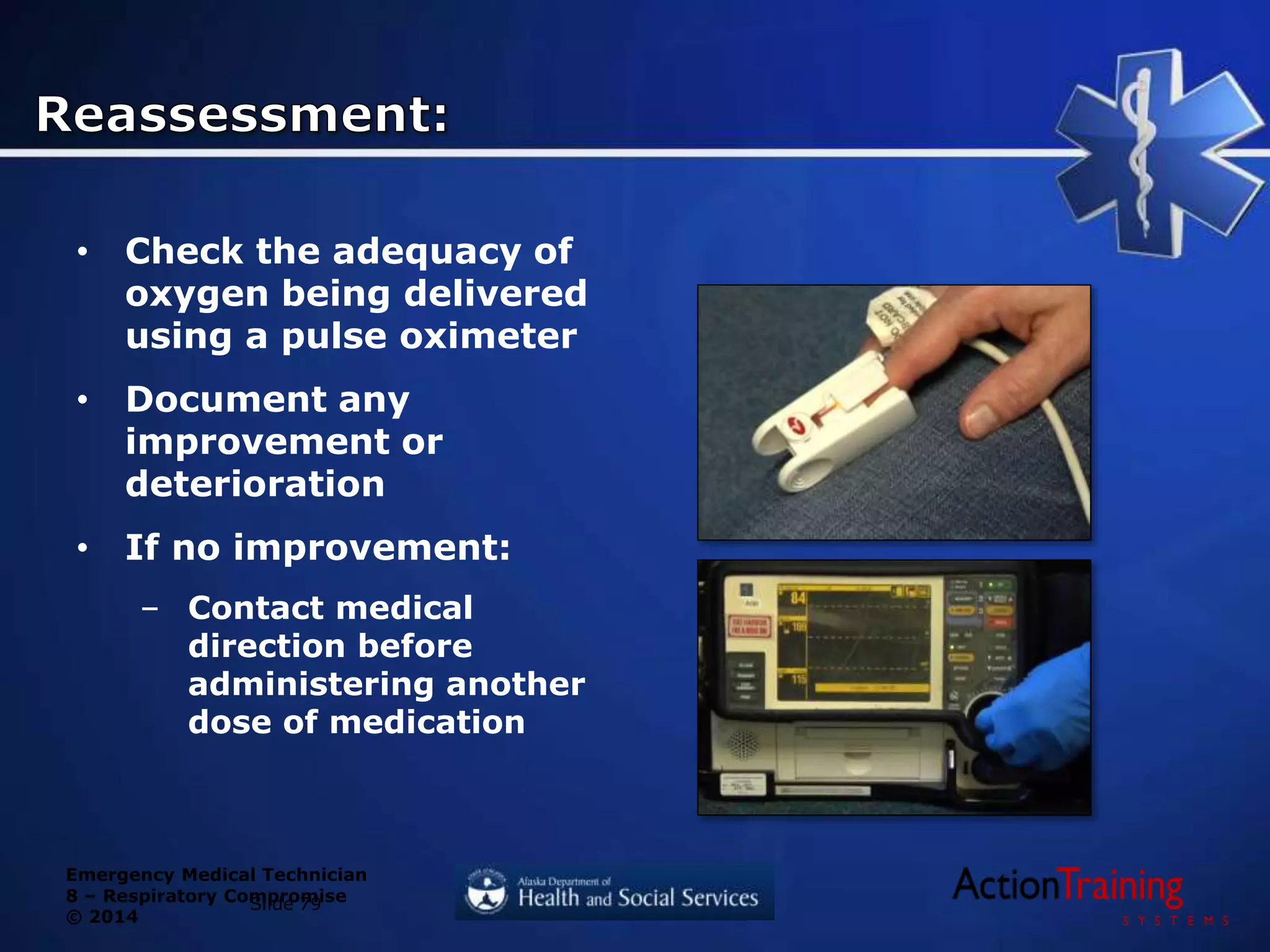

















The document discusses respiratory compromise, which occurs when the respiratory system becomes impaired, limiting oxygen intake and carbon dioxide expulsion. This can be caused by injuries, illnesses, or conditions affecting the airway, respiration, or ventilation. Common signs of respiratory compromise include abnormal breathing sounds, respiratory distress, changes in rate/rhythm, and altered mental status. EMTs must rapidly assess patients for adequate oxygenation and provide immediate intervention if breathing is inadequate, as respiratory failure can develop quickly and threaten life.



































































