Download as PDF, PPTX
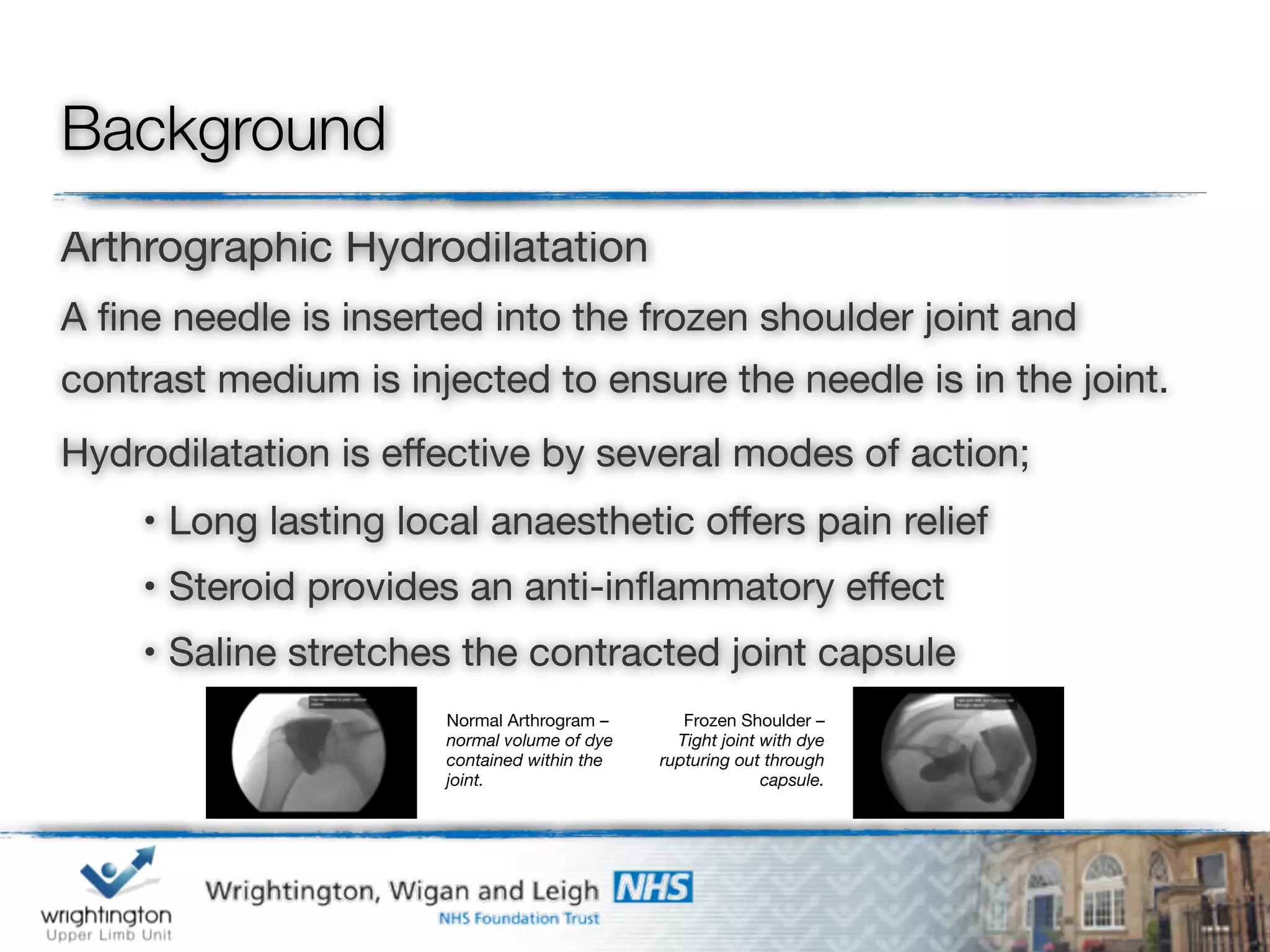



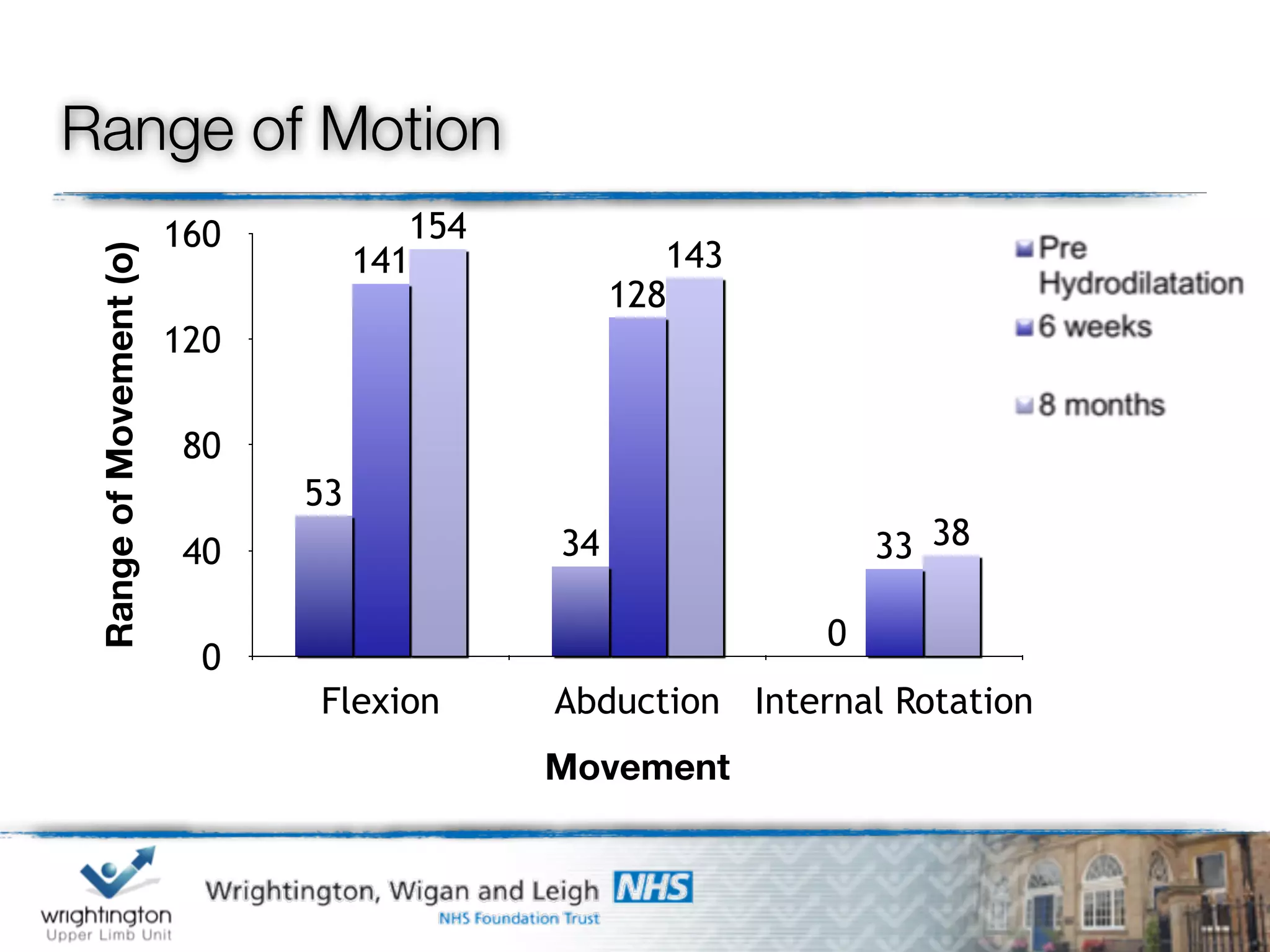





This document discusses arthrographic hydrodilatation as a treatment for frozen shoulder. Arthrographic hydrodilatation involves injecting local anesthetic, steroid, and saline into the frozen shoulder joint under imaging guidance to relieve pain and stretch the contracted joint capsule. A study of 51 patients found that arthrographic hydrodilatation significantly improved shoulder range of motion, pain levels, and outcome scores up to 8 months post-procedure, with 86% of patients satisfied. The procedure provides an effective non-surgical option for treating both primary and secondary frozen shoulder.











































































































