Downloaded 37 times

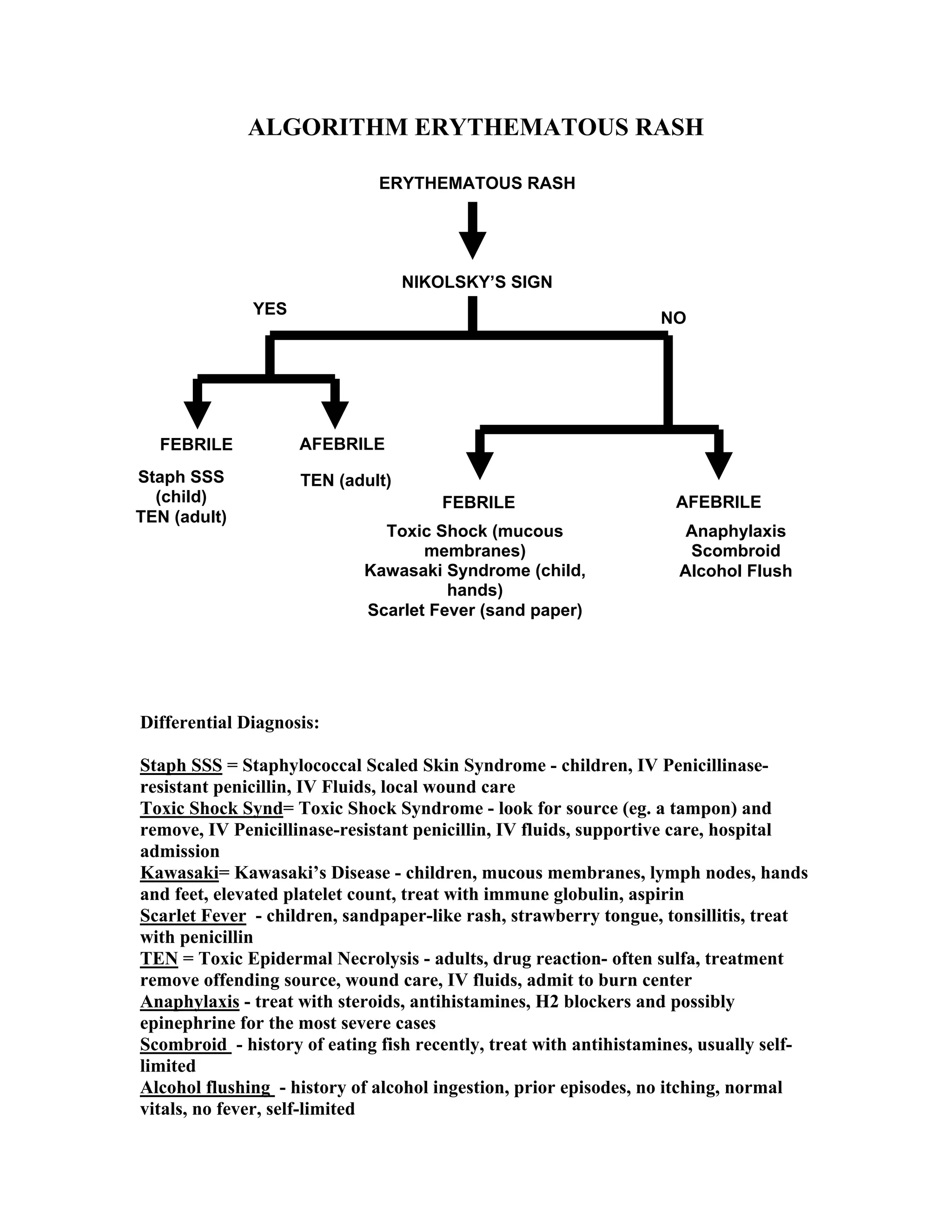


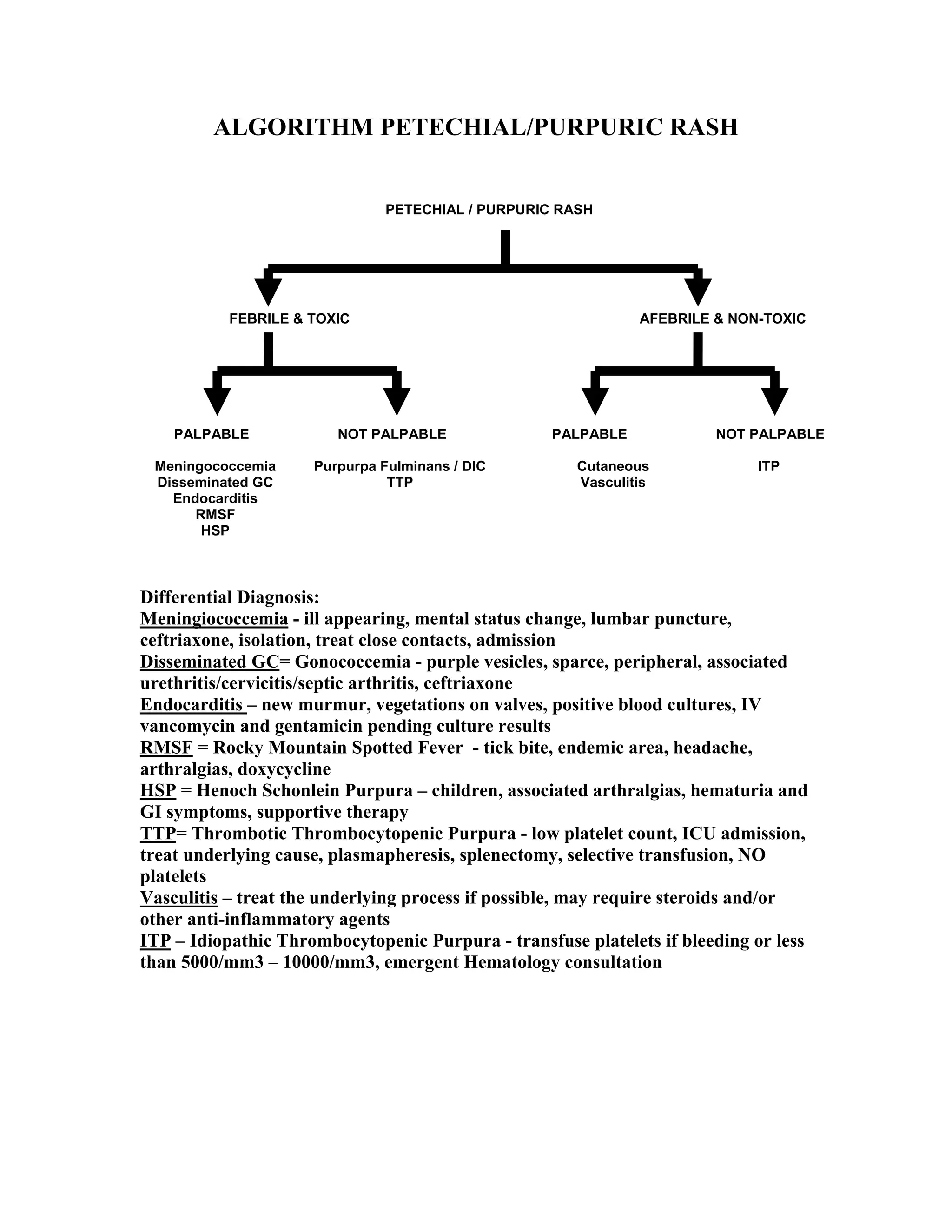
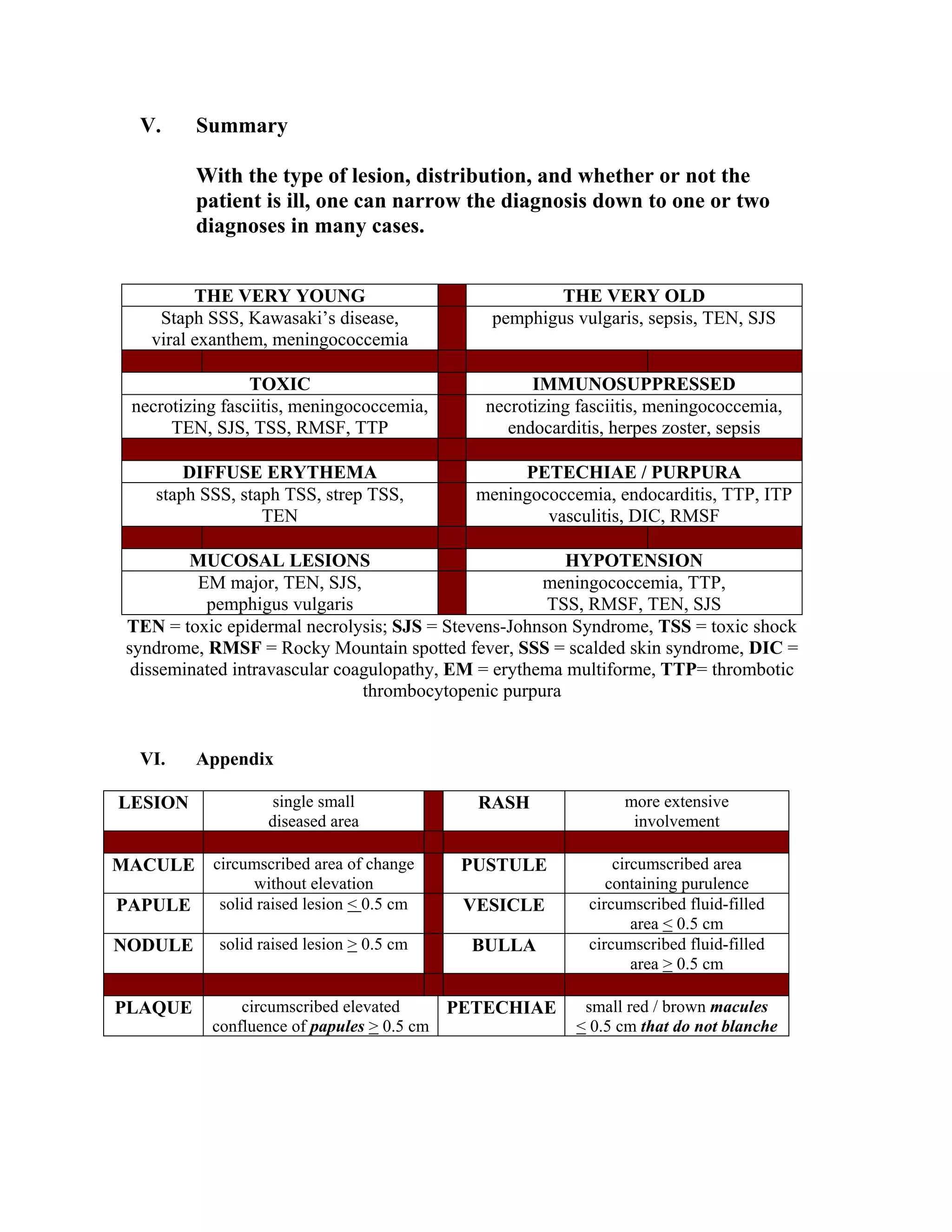



This presentation provides guidelines for systematically evaluating and diagnosing unknown rashes seen in the emergency department setting. [1] The speaker outlines a structured approach involving obtaining a thorough history, performing a focused physical exam describing the rash characteristics, and utilizing diagnostic algorithms to establish a differential diagnosis based on lesion type, distribution, and associated symptoms. [2] Key considerations include differentiating potentially life-threatening conditions requiring emergent interventions from self-limiting disorders. [3] Through a systematic approach, the unknown rash can often be narrowed down to one or two likely diagnoses to guide appropriate treatment and disposition.











































































































