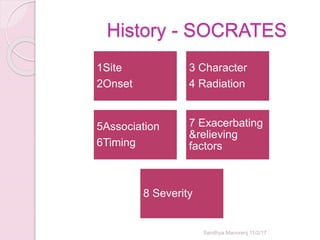
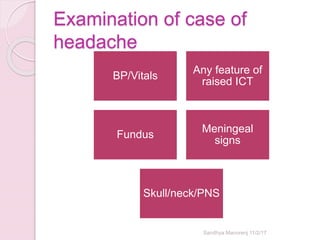
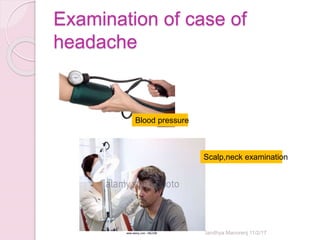
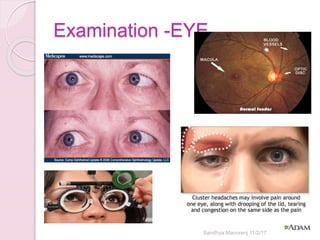
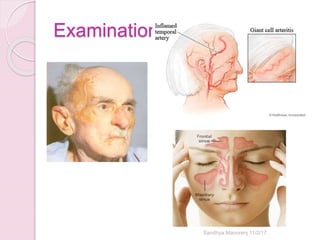
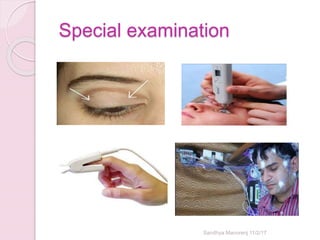
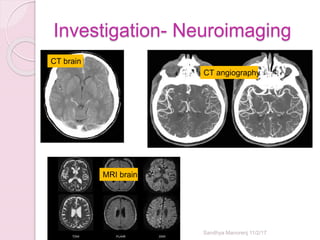
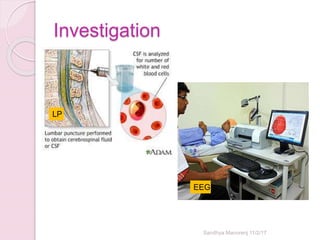
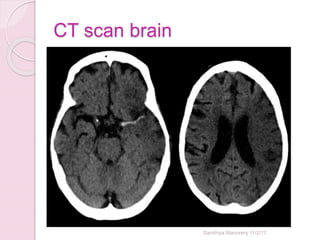
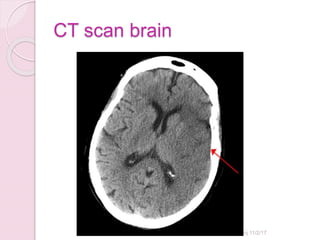
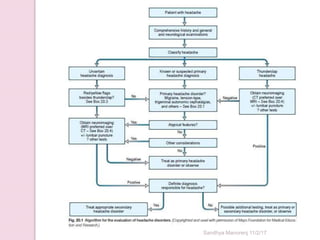
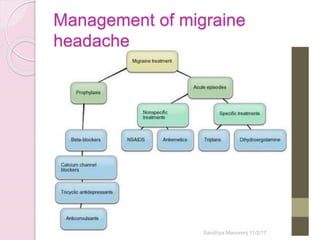
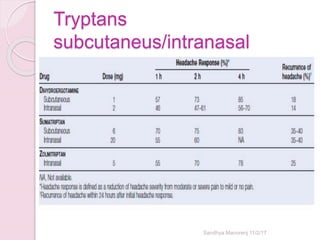
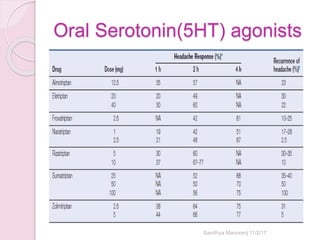
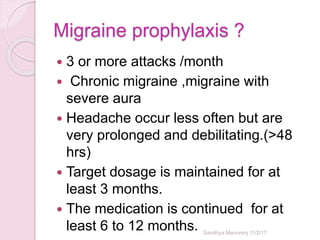
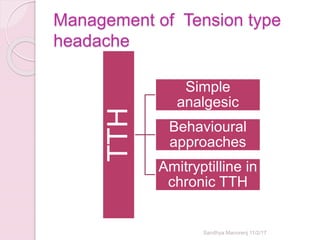
Dr. Sandhya Manorenj provides an overview of approaches to headache and migraine. Nearly half of adults worldwide have an active headache disorder. History taking follows the SOCRATES method and examination evaluates for signs of increased intracranial pressure. Investigation may include neuroimaging like CT or MRI to identify underlying causes. Treatment involves acute and preventative medications that vary depending on the headache type, like triptans for migraines or verapamil for cluster headaches.