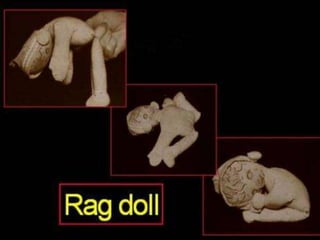
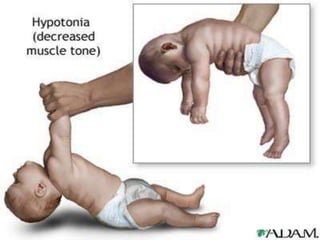
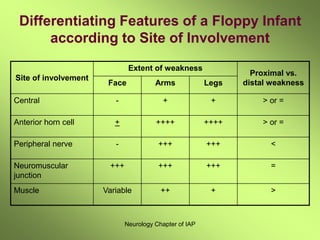
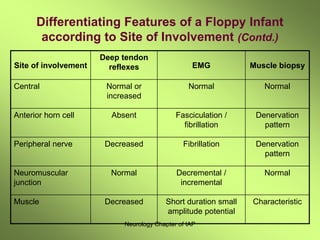
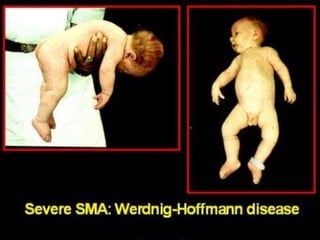
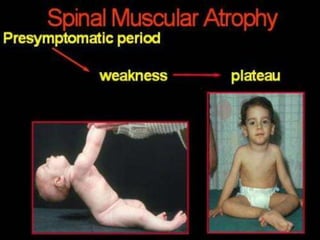
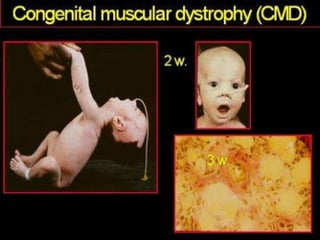
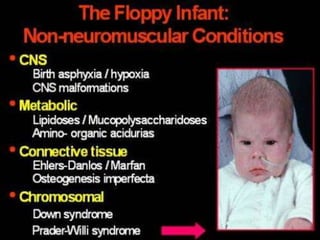
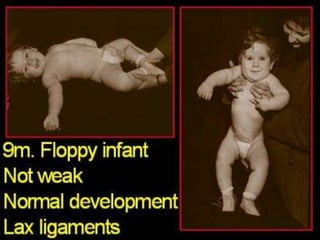
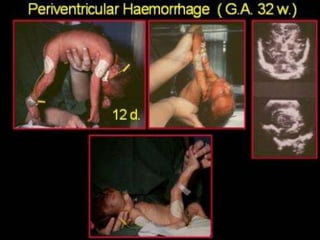
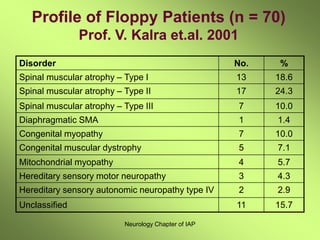
This document discusses the approach to evaluating and diagnosing a floppy infant. A floppy infant refers to one with generalized low muscle tone or hypotonia. Common causes discussed include central nervous system issues like cerebral palsy, lower motor neuron disorders like spinal muscular atrophy, and myopathies. The document outlines examination findings that can help localize the source of the hypotonia. Initial tests may include bloodwork and imaging while EMG, genetic testing, and muscle biopsy can further evaluate certain causes. The most common causes found in one study of floppy infants were various forms of spinal muscular atrophy and congenital myopathies.