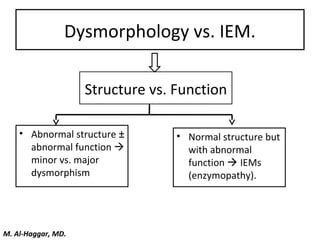





1. The document discusses an algorithmic approach to diagnosing malformed infants and children. It addresses dysmorphology versus inborn errors of metabolism, the importance of history and examination findings, and classifications of malformations. 2. Key classifications discussed include deformations, disruptions, dysplasias, and malformation syndromes. Flow charts are provided to guide clinicians through assessing number of malformations, tissues involved, tissue damage, and joint/bone involvement to determine classification. 3. Examples are given to demonstrate the application of the algorithm, such as identifying achondroplasia as a skeletal dysplasia based on involvement of one tissue with intact bones and joints. The importance of a systematic approach and differential diagnosis























































































