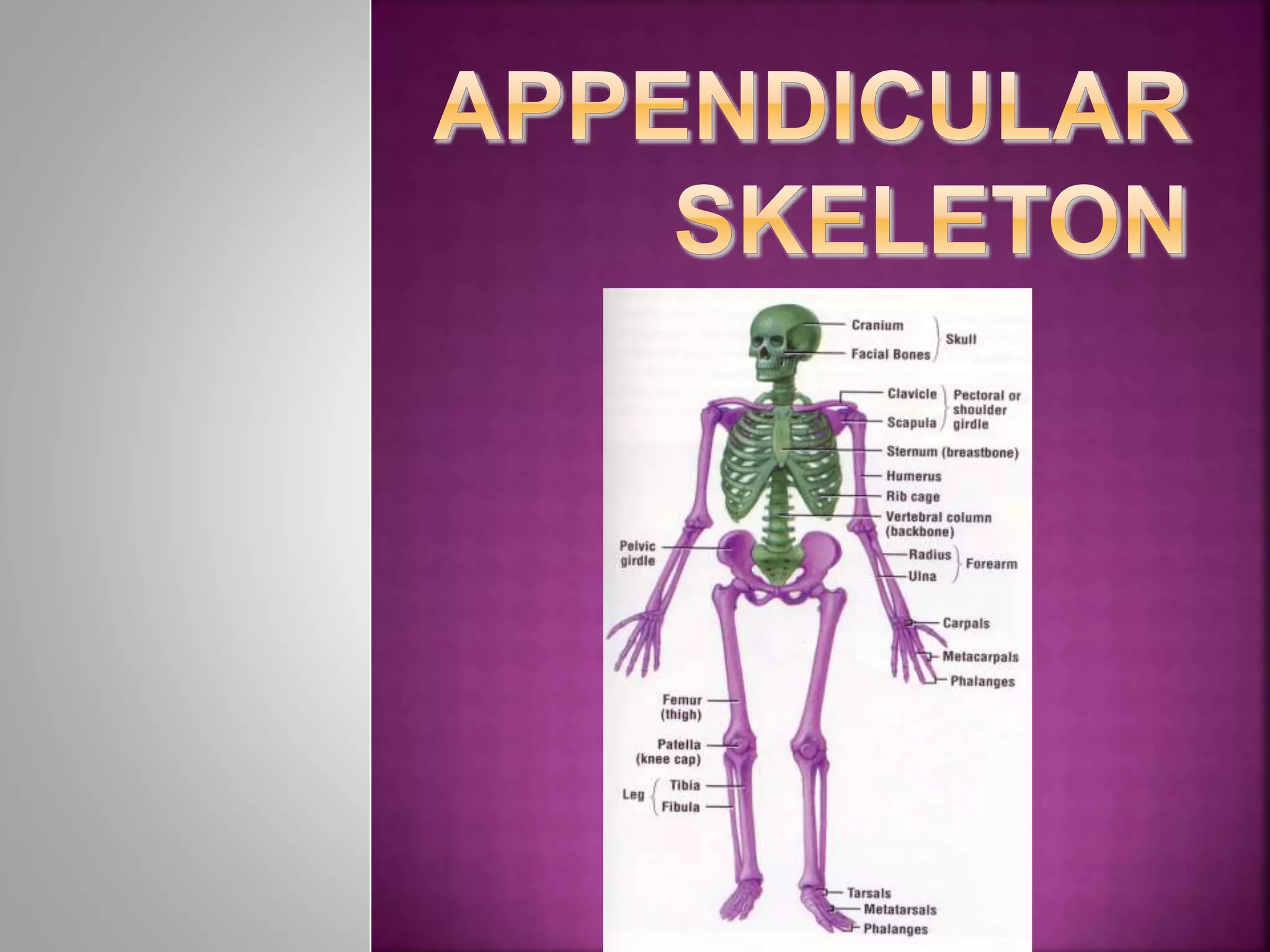
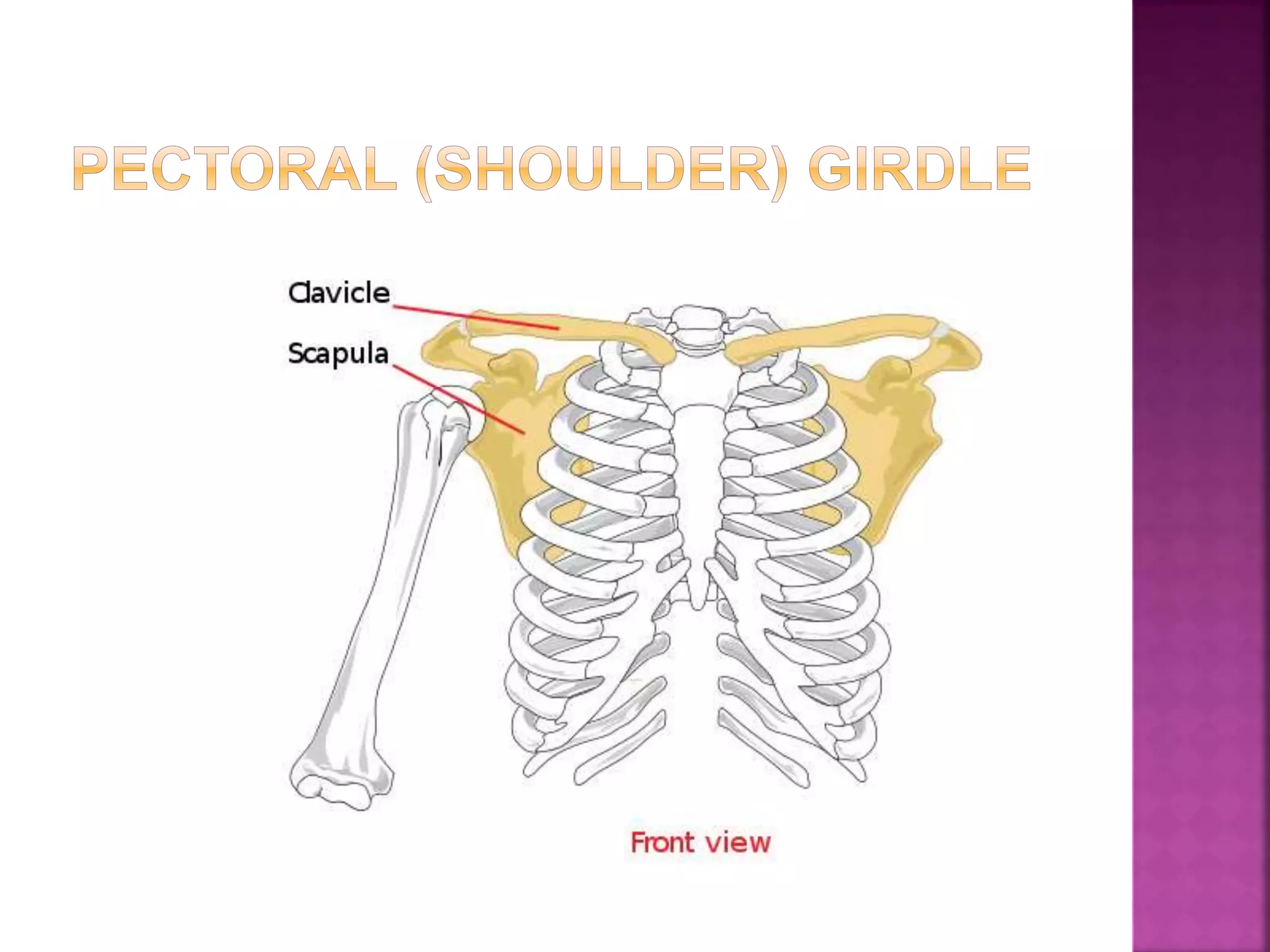
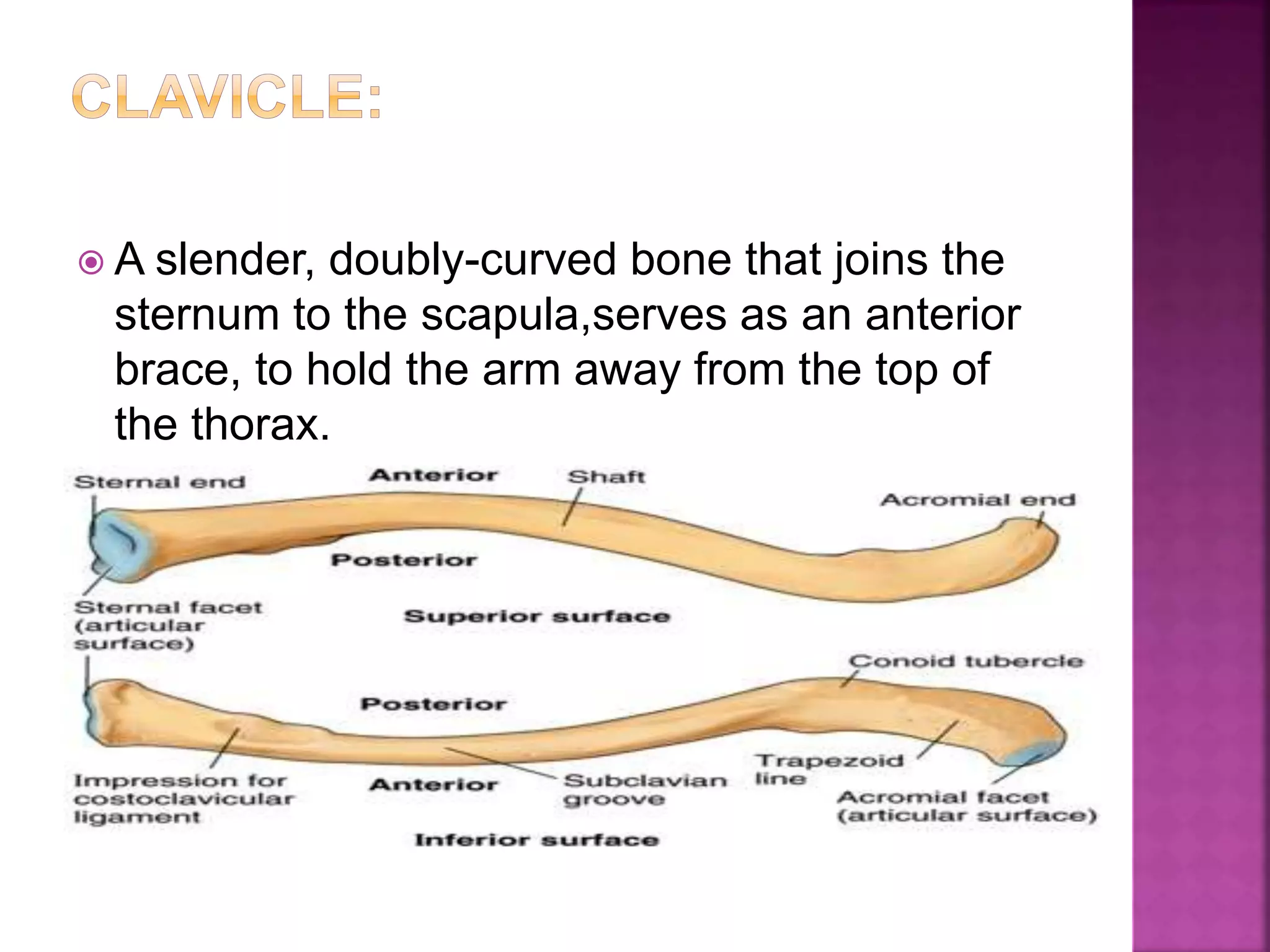
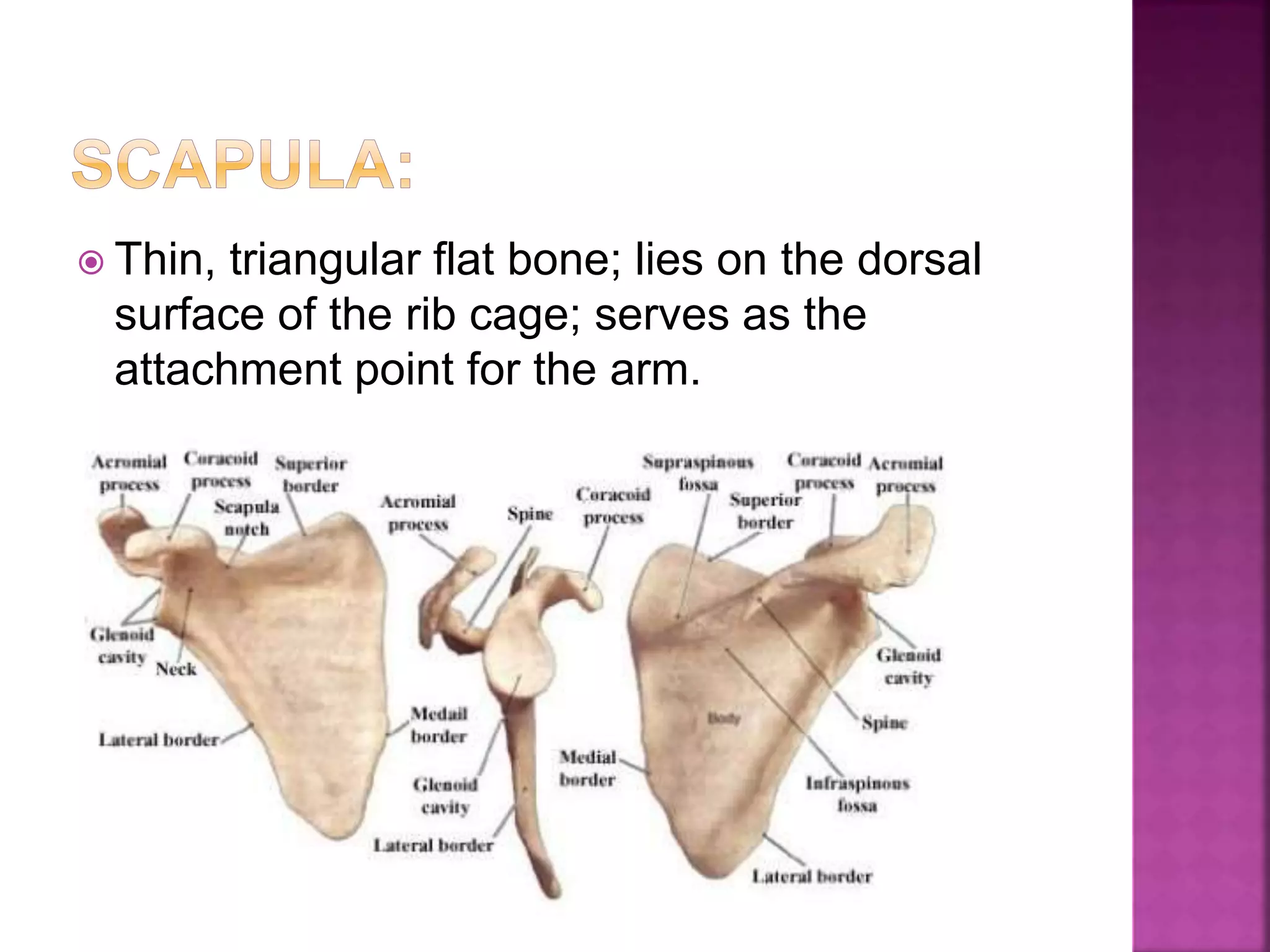
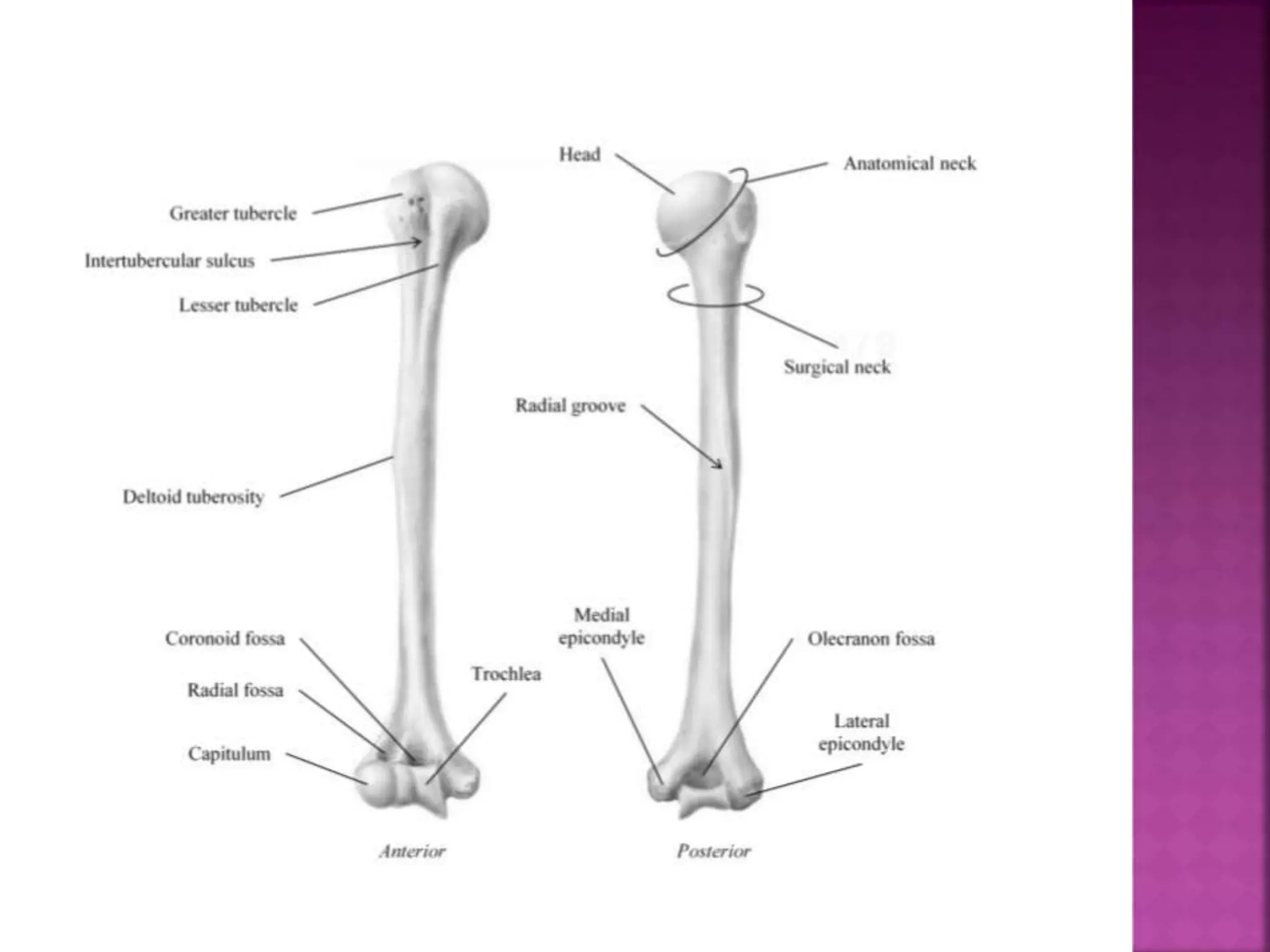
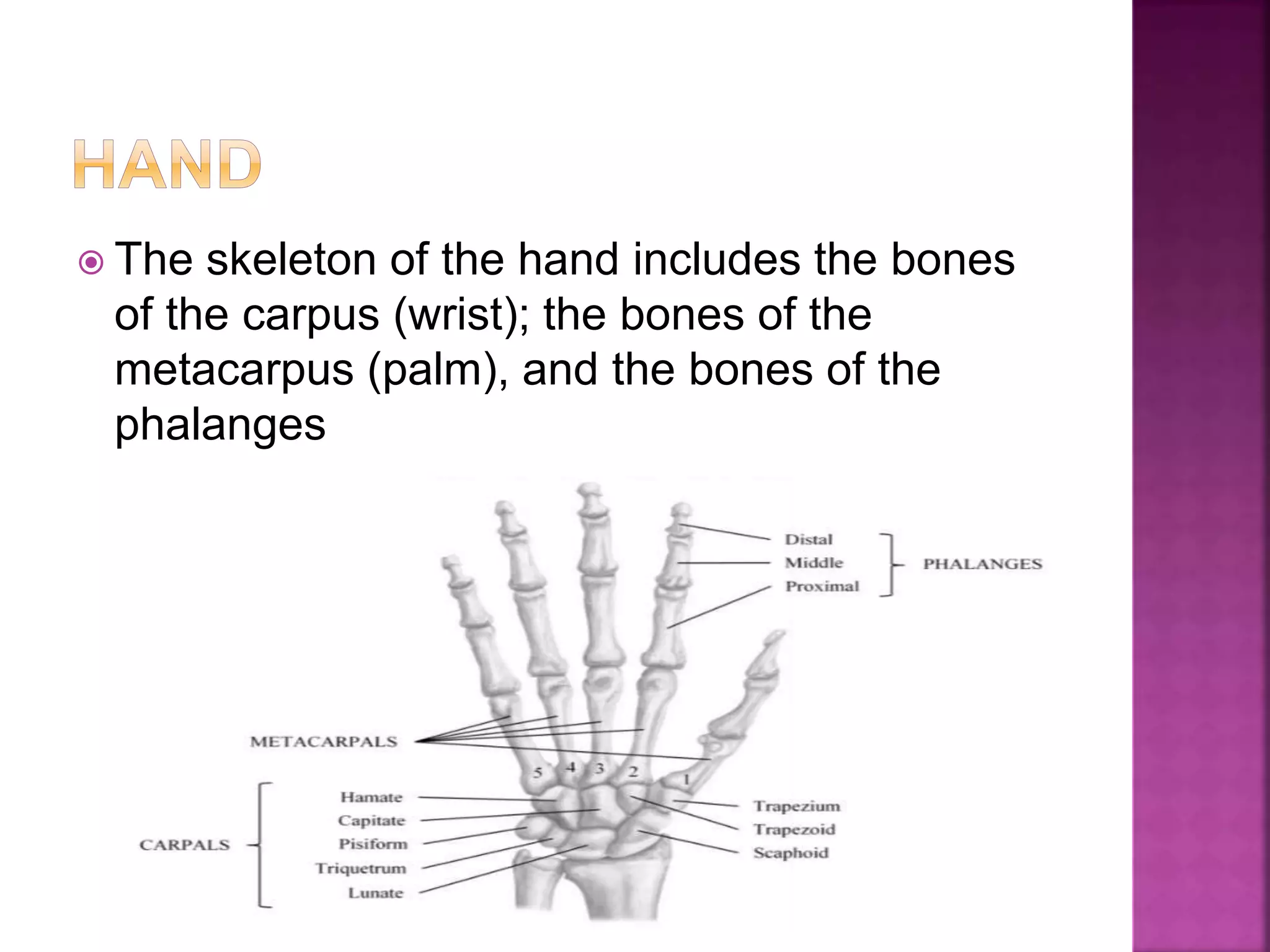
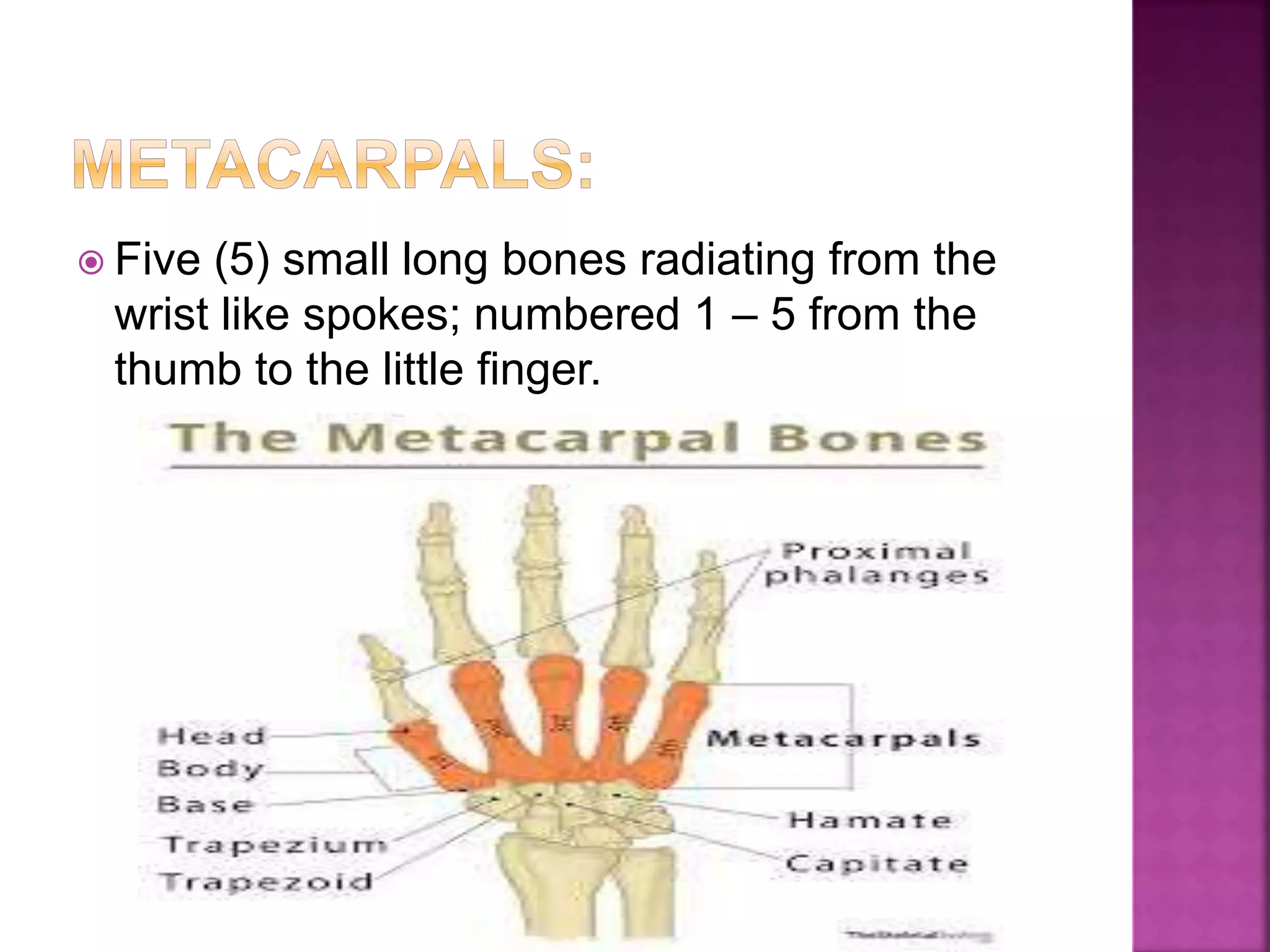
The document summarizes the bones that make up the pectoral girdle, upper limb, forearm, and hand. It describes the clavicle and scapula bones that form the shoulder girdle and their landmarks. It then discusses the humerus bone of the upper arm, and the radius and ulna bones of the forearm. Finally, it briefly outlines the carpal bones of the wrist, metacarpal bones of the palm, and phalanges bones of the fingers.