Download to read offline

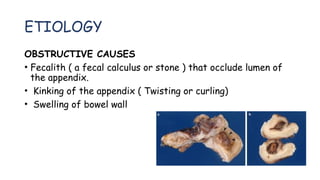
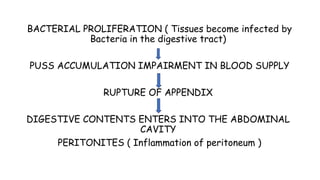
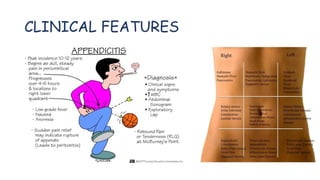
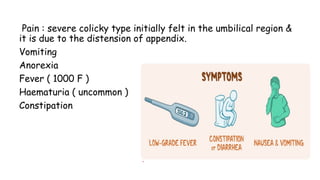

Appendicitis is an inflammation of the appendix, characterized by severe pain in the lower right abdomen, most commonly affecting individuals aged 10 to 30. It can result from obstructive causes like fecalith and swelling, leading to complications such as rupture and peritonitis if untreated. Surgical removal (appendectomy) is the standard treatment, with laparoscopic procedures being less painful and leading to quicker recovery.











































![APPENDICITIS Nursing managment[Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/appendicitisautosaved-250207063037-951fd6a3-thumbnail.jpg?width=640&height=640&fit=bounds)
































