ANATOMY & PHYSIOLOGY
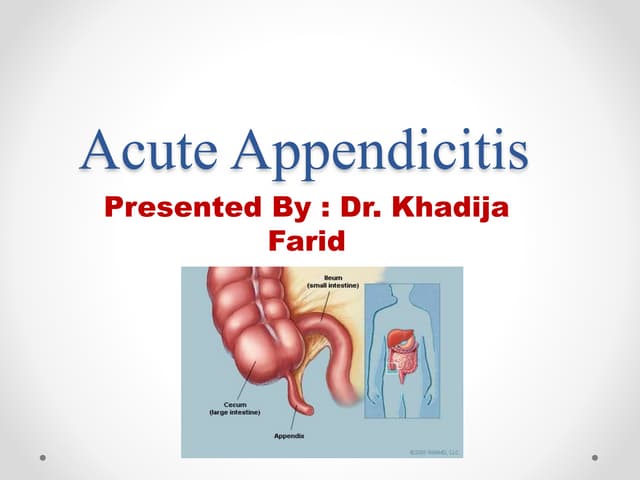
•The appendix sits at the junction of the small intestine and large
intestine.
• It's a thin tube about four inches long. Normally, the appendix sits
in the lower right abdomen.
3.
DEFINITION
• Appendicitis isan inflammation of the vermiform appendix that
develops most commonly in adolescentsand young adults.
• Appendicitis is an acute inflammation of theappendix.
4.
ETIOLOGY
OBSTRUCTIVE CAUSES
-Fecalith (a fecal calculus or stone) that occlude lumen of the appendix.
- Kinking of the appendix (Twisting or curling)
- Swelling of bowel wall
NON OBSTRUCTIVE CAUSES
-Haematogenous spread of infection
- Vascular occlusion
- Trauma
-Diet lacking fibres
CLINICAL FEATURES
SYMPTOMS
• Pain:severe colicky type initially felt in the umbilical region
& it is due to the distension of appendix.
• Vomiting
• Anorexia
• Fever ( 100° F)
• Haematuria (uncommon)
• Constipation
PSOAS'S SIGN
• Psoassign is right lower-quadrant pain that is produced with
the patient extending the hip due to inflammation of the
peritoneum. Straightening out the leg causes the pain because
it stretches the muscles.
11.
ROVSING'S SIGN
•The Roving'ssign is positive when pressure over the
patient's left lower quadrant causes pain in the rightlower
quadrant.
12.
OBTURATOR'S SIGN
• Painon passive internal rotation of the flexed thigh. Examiner
moves lower leg laterally while applying resistance to the lateral
side of the knee resulting in internal rotation of the femur.
13.
BLOOMBERG'S SIGN
• BLOOMBERG'SSIGNAlso referred as rebound tenderness.
• Deep palpation of the viscera over the suspected inflamed appendix
followed by sudden release of the pressure causes the severe pain on
the site.
• This indicates positive Blumberg's sign peritonitis.
14.
MCBURNEY'S SIGN
• McBurney's Point is two third away from umbilicus to Anterior
superior iliac spine
• To elicit Mcburney's sign patient should be in supine position with
his knees slightly flexed and his abdominal muscles relaxed.
• Palpate deeply and slowly in the right lower quadrant over
McBurney's point ,located about 2" from the Rt.Ant. Sup. Iliac
Spine, On a line between the spine and umbilicus.
• pain and tenderness is a positive sign and indicates appendicitis.
15.
Aaron sign isa clinical sign that is defined as a feeling of
distress and pain in the epigastric, umbilical and
praecordial regions, on steady pressure over McBurney
point, it is suggestive of chronic appendicitis.
DUNPHY’S SIGN
Dunphy's sign is a medical sign characterized by
increased abdominal pain with coughing – may be an
indicator of appendicitis.
AARON’S SIGN
16.
•Others include
Cough tenderness
Indicateinflammation of Parietal Peritoneum
• Guarding and Rigidity
Present in the right iliac fossa.
• Rectal examination
There is tenderness in the right rectal wall
• PerVaginal Examination
Presence of ovarian mass, tenderness on movement of cervix.
17.
M U RP HY ' S TRIAD
Pain first, Followed by vomiting and then fever is called Murphy's
traid of syndrome of appendicitis ( Murphy's Syndrome)
18.
CLINICAL STAGES
• Thestages of appendicitis can be divided into early,
suppurative, gangrenous.
• Early stage appendicitis
-In the early stage of appendicitis, obstruction of the appendiceal
lumen leads to
>Mucosal edema
>mucosal ulceration
>bacterial diapedesis
>appendiceal distention due to accumulated fluid, and
increasing intraluminal pressure.
19.
oThe visceral afferentnerve fibers are stimulated, and the patient
perceives mild visceral periumbilical or epigastric pain, which usually
lasts four to six hours.
• Suppurative appendicitis
• Increasing intraluminal pressures eventually exceed capillary
perfusion pressure.
• Transmural spread of bacteria causes acute suppurative appendicitis.
• When the inflamed serosa of the appendix comes in contact with the
parietal peritoneum, patients typically experience the classic shift of
pain from theperiumbilicus to the right lower abdominal
quadrant(RLQ), which is continuous and more severe than the early
visceral pain.
DIAGNOSTIC MEASURES
• Historycollection
• Physical examination
• White cell count (WCC) - usually mildly elevated, around 11-14,000
• C reactive protein (CRP) - elevated.
• Urinalysis
• Complete blood count
• CT- Scan
• Ultrasound - visualise tubular structures & cysts
• USG is not accurate as CT sometimes difficult to see appendix
• Magnetic resonance imaging
• x-ray
Medical Management
Goal ofmedical management includes
• To treat infections
• To prevent further complications
• Medication therapy includes
-Antibiotic therapy – eg- cephalosporin
-Anti inflammatory drugs – eg- Metrogyl
-Analgesics
-Fluid therapy
24.
SURGICALMANAGEMENT
• The surgicalprocedure for the removal of the appendix is
called an appendectomy.
•Appendectomy can be performed through open or
laparoscopic surgery.
• Laparoscopic appendectomy has several advantages over open
appendectomy as an intervention for acute appendicitis.
25.
Appendicecotmy
• Appendicectomy isa surgical procedure to remove the appendix from
the abdomen. It can be performed either with a small incision on the
abdomen or laparoscopically (key hole surgery).
• Indications for open appendicectomy
- Dense adhesions due to inflammation or prior surgical procedures.
- Perforated or gangrenous appendicitis.
- Generalized peritonitis.
26.
Pre- operative Preparation
•Once diagnosis is suspected, the Patient is Admitted to
hospital.
• IV Fluid s- isotonic Saline or Ringer lactate is given.
•Ryle's tube is not necessary in simple appendicitis.
• Second generation Cephalosporin along with metronidazole is
given.
• Informed consent is taken.
27.
OpenAppendicectomy
• Incision (transverse,Mc Burney's point)
• Open in layers. (muscle is split along its fibres)
• Check for fluid (+/-c&S)
• Identify caecum and exteriorized - follow taeniae to appendix
• Mesoappendix divided + ligated
• Clamp appendix 5mm above caecum and ligated
• Cauterise residual mucosa +/- purse string (not req)
• Return caecum, wash with warm saline
• Close in layers
28.
Lap.Appendicectomy
• Become popularnowadays
• Less post operative pain
• Speedy recovery
If intraoperative complications that cannot behandled withhandled
with laparoscopy arise duringlaparoscopic appendectomy,
conversion to an open appendectomy
29.
LaparoscopicAppendicectomy
• Usu 3ports. 1 umbilical, 1 suprapubic (12mm)and 1 rt periumb
region (anatomy) (5mm)
• Pneumoperitoneum (10-14mmHg)
• Appendix is grasped and retracted up toexpose mesoappendix >
divided -> ligated
• Appendix transacted and delivered inendobag
• Peritoneal irrigation
• Closure of fascia and skin
34.
Investigations
• Routine bloodtests
-Todetermine an increase in leukocytes is a sign of infection.
• Abdominal examination
-To know the existence of post-surgical complications.
35.
COMPLICATIONS
• Appendicitis cancause serious complications, such as
- A ruptured appendix.
- Arupture spreads infection throughout abdomen (peritonitis) - life-threatening.
- this condition requires immediate surgery t0 remove thw appendix
• A pocket of pus that forms in the abdomen.
- If appendix bursts, Patient may develop a pocket of infection (abscess).
- In most cases, a surgeon drains the abscess by placing a tube through abdominal
wall into the abscess site
-The tube is left in place for two weeks,
-Antibiotics are given to clear the infection
36.
How to differentiatean appendicular lump
and an appendicular abscess?„
In a classical case
-The appendicular lump - forms around the third day of acute
attack of pain and develops into an abscess around fifth to tenth
day.„
-Pyrexia, aggravation of the local signs and a rising leukocyte
count are indicators of abscess formation.„
-USG and CT scan may demonstrate pus within an appendicular
lump.
37.
conservative treatment forappendicular lump?
(Ochsner’s Sherren regime) „
- For pain: nonsteroidal anti-inflammatory drugs (Diclofenac or aceclofenac) or narcotic analgesics
(Injection pentazocine or pethidine).„
- For vomitting: Stop oral fluids, nasogastric suction.„
- Fluid administration: Intravenous fluids to maintain fluid electrolyte balance.
If patient is not vomiting—oral fluids may be administered.„
- Control infection: 2nd or 3rd generation cephalosporin
(Cefuroxime or ceftriaxone) along with metronidazole administered parenterally.Alternatively a
combination of Ampicillin + Gentamycin + Metronidazole may be given.„
- Monitoring is the most important component of conservative treatment:
• Symptomatic improvement—pain, vomiting.
• objective improvement:− Hourly monitoring of pulse, blood pressure and respiration.
• Monitoring of temperature 4 hourly.
• Tenderness in right iliac fossa.
• Progress of the lump (lump is to be marked)
If the patient responds well to conservative treatment, interval appendicectomy should be considered
after 6–8 weeks.
38.
CONCLUSION
Appendicitis is aninflammation of the appendix, a finger-shaped
pouch that projects colon on the lower right side of your
abdomen.Appendicitis causes pain in your lower right abdomen.
However, in most people, pain begins around the navel and then
moves.As inflammation worsens, appendicitis pain typically
increases and eventually becomes sever.
























































![APPENDICITIS Nursing managment[Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/appendicitisautosaved-250207063037-951fd6a3-thumbnail.jpg?width=640&height=640&fit=bounds)