Downloaded 115 times

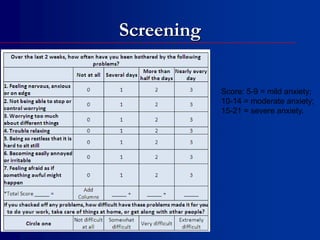


The document discusses anxiety disorders, specifically generalized anxiety disorder (GAD). It notes that primary care physicians treat 60% of patients with panic and anxiety disorders, but 90% of cases have been undiagnosed. GAD has a lifetime prevalence of 5% in American adults and involves excessive, uncontrollable worry about multiple events for at least 6 months. Treatment options for GAD include SSRIs, SNRIs, benzodiazepines, buspirone, cognitive behavioral therapy, and augmenting SSRIs with bupropion or pregabalin. The document also provides screening tools and discusses managing GAD with comorbid depression.






































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)








![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

