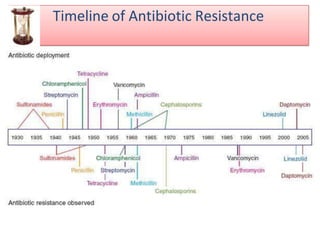
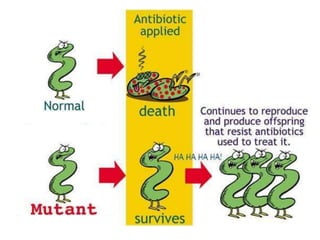
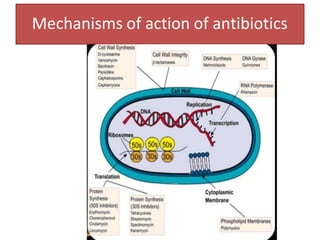
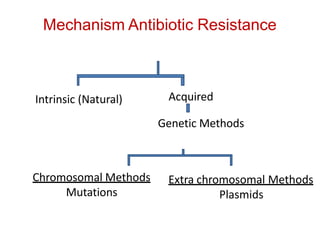
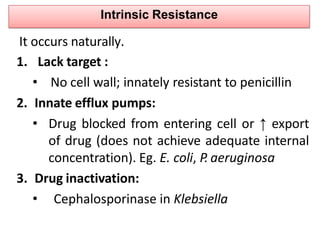
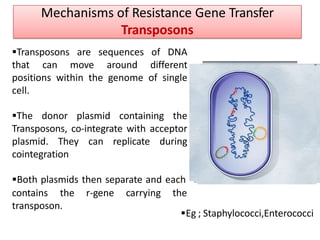
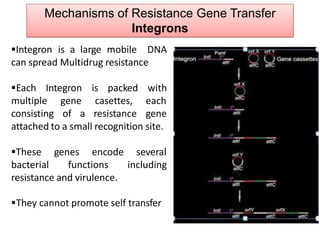
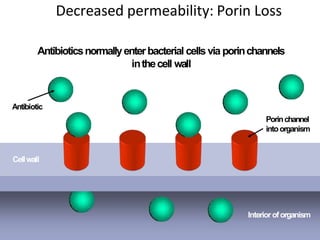
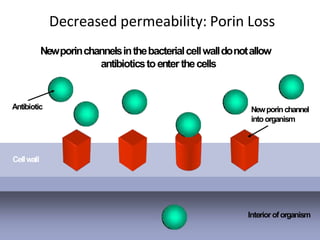
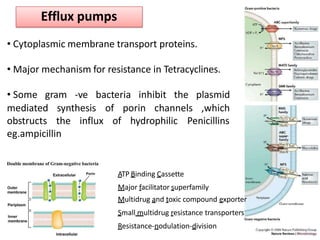
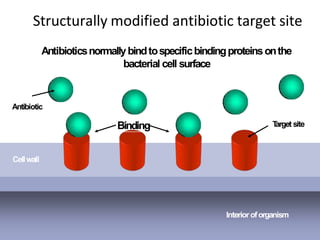
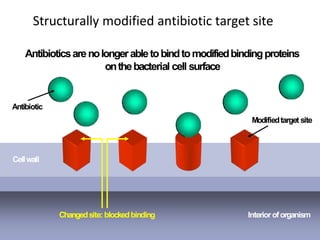
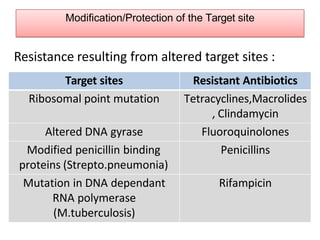
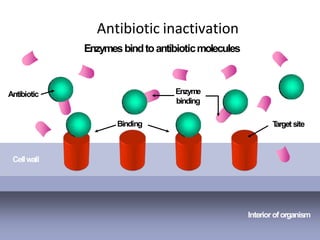
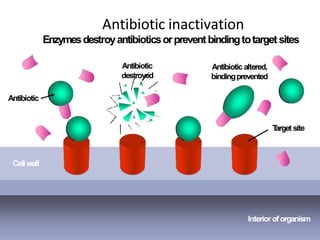
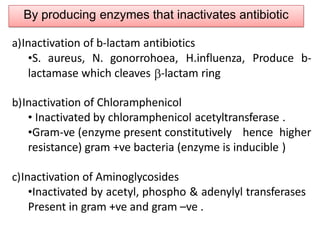
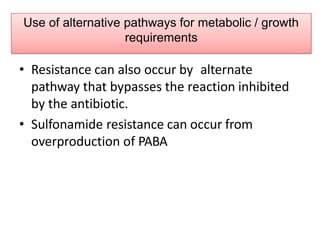
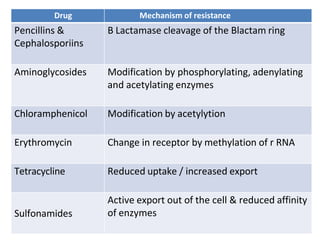
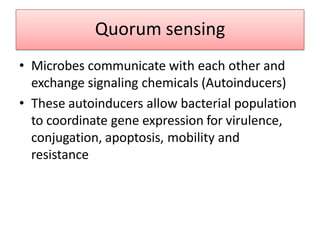
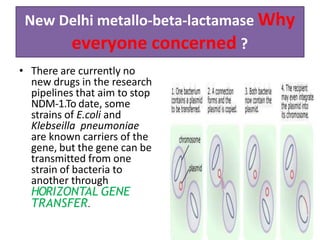
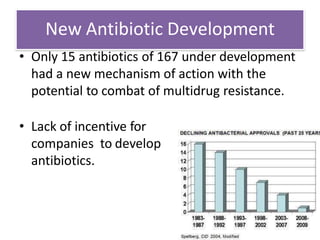
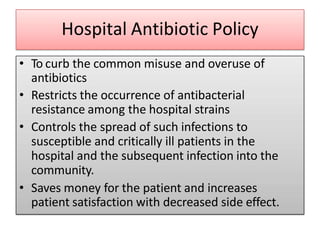
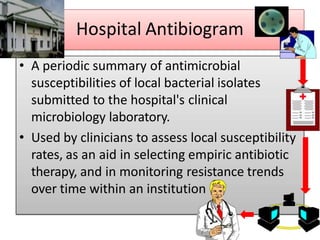
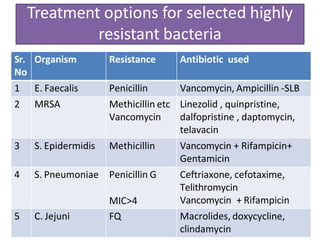
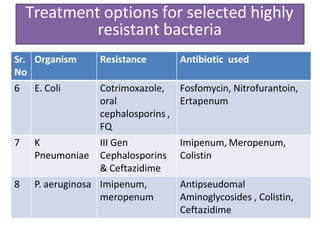
The document discusses the problem of antibiotic resistance and strategies to contain it. It provides background on antibiotic resistance, describing how it can occur intrinsically in bacteria or be acquired through mutations, plasmids, or gene transfer. Various mechanisms of resistance are outlined, including decreased permeability, efflux pumps, target modification, and antibiotic inactivation. The Indian scenario highlights specific resistance issues. NDM-1 carbapenemase is described as a major concern due to its ability to spread. Containment strategies include developing new antibiotics, judicious antibiotic use, and infection control.


























































![عيادةالاسنان [Autosaved].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/autosaved-230717125803-9c04fe38-thumbnail.jpg?width=640&height=640&fit=bounds)







![stirlization - Copy [Recovered].ppsx](https://cdn.slidesharecdn.com/ss_thumbnails/stirlization-copyrecovered-221212090857-e0153d3b-thumbnail.jpg?width=640&height=640&fit=bounds)



![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
















![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)