Organization of theNervous System
Two principal divisions of the nervous system:
1.Central nervous system (CNS) consists of the brain and
spinal cord. Within the CNS, various sorts of incoming
sensory information are integrated and correlated.
2. Peripheral nervous system (PNS) includes 12 pairs of
cranial nerves that arise from the brain and 31 pairs of
spinal nerves that emerge from the spinal cord.
The CNS is connected to sensory receptors, muscles, and
glands in peripheral parts of the body by the PNS
4.
Peripheral nervous systemsubdivided into two parts:
(based on body area response)
1. Somatic: body
2. Autonomic: smooth muscle, cardiac muscle, glands
Somatic consists of sensory neurons that convey
information from cutaneous and special sense receptors
primarily in the head, body wall, and extremities to the
CNS and motor neurons from the CNS that conduct
impulses to skeletal muscles only.
5.
Autonomic nervoussystem consists of sensory
neurons that convey information from receptors
primarily in the viscera (internal organs) to the
CNS and motor neurons from the CNS that
conduct impulses to smooth muscles, cardiac
muscle, and glands.
Motor portion of the ANS consists of two
branches:
1. Sympathetic
2. Parasympathetic
6.
Neurons are thebasic unit of the nervous system. They
carry information or impulses as electrical signals from
one place to another in the body. There are 3 types of
neurons:
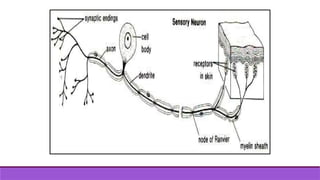
Sensory Neurons- Sensory neurons carry electrical signals
(impulses) from receptors or sense organs to the CNS.
Sensory neurons are also called afferent neurons. The cell
body of sensory neurons is outside the CNS in ganglia.
8.
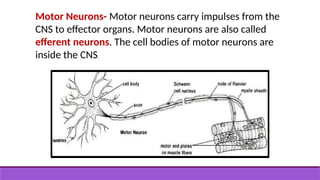
Motor Neurons- Motorneurons carry impulses from the
CNS to effector organs. Motor neurons are also called
efferent neurons. The cell bodies of motor neurons are
inside the CNS.
9.
Interneurons- These arealso called intermediate,
relay, or associative neurons. They carry information
between sensory and motor neurons. They are found
in the CNS.
10.
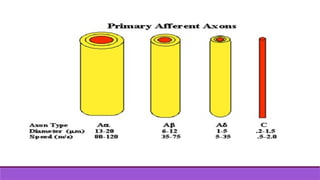
Types of nervefibers:
The information about touch and other sensation is
transmitted to the spinal cord and brain by nerve
fibers that are connected to the different types of
receptors in the skin, muscle and internal organs.
These fibers come in different diameters and
consequently different functions There are two
main classification of nerve fibers which we must
know as they are both in general use.
11.
General classification ofnerve fibers
In the general classification the fibers are divided into three
main types:
- A Fibers: Large myelinated, fast conducting, motor
and sensory nerve fibers. Group A are divided into
alpha (a), beta (b), gamma (g), and delta (d) neurons.
- .
12.
- B Fibers:Smaller and slower conducting myelinated,
efferent, preganglionic fibers of the autonomic nervous
system.
- C Fibers: Unmyelinated post-ganglionic fibers of the
sympathetic nervous system unmyelinated or poorly
myelinated afferent fibers of the peripheral nerves.
Group C fibers are small and slow conducting
14.
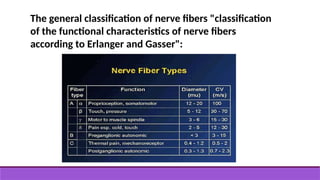
The general classificationof nerve fibers "classification
of the functional characteristics of nerve fibers
according to Erlanger and Gasser":
pain:
an unpleasant sensoryand emotional experience associated
with actual or potential tissue damage‘.
Thus pain has objective, physiologic sensory aspects as well as
subjective emotional and psychological components In
consequence, the perception of pain and its threshold are the
result of complex interactions between sensory, emotional,
and behavioral factors.
17.
What is thepurpose or function of pain?
Protective function:
A withdrawal reflex response to an acute noxious stimulus is
an understandable and necessary reaction that has an
obvious protective function even in the absence of
conscious perception.
18.
Biological function:
•More importantly, the experience of pain may lead
to the avoidance of potentially harmful situations
and possible injury.
• Immobility and withdrawal due to pain may serve
to provide an environment in which healing and
restoration of function can occur.
19.
Nociceptive Processing
The physiologiccomponent of pain is termed nociception,
which consists of the following processes:
• Ttransduction
• Ttransmission
• Perception
• Mmodulation of neural signals generated in response
to an external noxious stimulus.
21.
Transduction
Transduction isthe process by which afferent nerve
endings participate in translating noxious stimuli (e.g., a
pinprick) into nociceptive impulses.
Nociceptors are receptors that are sensitive to noxious
or painful stimuli.
22.
Nociceptors are furtherclassified into four types:
1. The first type is termed high threshold
mechanonociceptors or specific nociceptors.
These nociceptors respond only to intense
mechanical stimulation such as pinching, cutting or
stretching.
2. The second type is the thermal nociceptors, which
respond to the intense heat and cold.
23.
3. The thirdtype is chemical nociceptors, which
respond only to chemical substances.
4. A fourth type is known as polymodalnociceptors,
which respond to high intensity stimuli such as
mechanical, thermal and to chemical substances like the
previous three types.
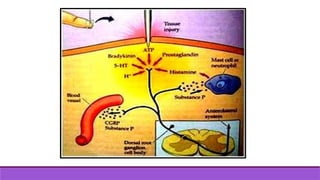
24.
Transduction
begins whenthe free nerve endings (nociceptors) of C fibres
and A- delta fibres of primary afferent neurones respond to
noxious stimuli.
More specifically, following tissue injury, chemical mediators
such as (substance P, cholecystokinin, acetylcholine,
prostaglandin, and bradykinin) are released to the vicinity of
nociceptors that may be activated and sensitized.
25.
The resultant"soup" of chemical mediators also changes
the transduction sensitivity of nociceptors, resulting in
reduction of threshold for activation and increased
response to suprathresholdstimulus,i.e., peripheral
sensitization.
27.
Transmission
Transmission is theprocess by which impulses are
sent to the dorsal horn of the spinal cord, and then
along the sensory tracts to the brain.
The transmission process occurs in three stages.
28.
1-The pain impulseis transmitted from the site of
transduction along the nociceptor fibers to the dorsal
horn in the spinal cord
Pain impulses are transmitted by two fiber systems:
- Aδ fibers are myelinated, 2 – 5 μm in diameter
and conduct at rates of 12 – 30 m/s,
-C fibers are unmyelinated, 0.4 – 1.2 μm in diameter
and conduct at rates of 0.5 to 2 m/s.
29.
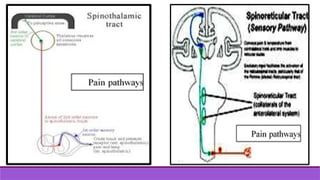
2-From the spinalcord to the brain stem and thalamus.
The fibers cross to the opposite side of the spinal cord,
and then ascend to brain stem and thalamus via the
anterolateral system which actually contains at least two
pathways:
-The first is called the spinothalamic pathway.
The most direct route to the thalamus, it is also known as
the neospinothalamic or direct pathway for fast pain.
30.
-The secondis known as the spinoreticular pathway
- also called the paleospinothalamic or indirect path
for slow pain.
The presence of two pain pathways explains the existence
of two components of pain: fast, sharp and well localized
sensation (first pain) which is conducted by Aδ fibers;
a duller slower onset and often poorly localized
sensation (second pain) which is conducted by C fibers
Perception
Perception of painis the end result of the neuronal activity
of pain transmission and where pain becomes a conscious
multidimensional experience.
The multidimensional experience of pain has affective-
motivational, sensory- discriminative, emotional and
behavioural components.
When the painful stimuli are transmitted to the brain stem
and thalamus, multiple cortical areas are activated and
responses are elicited.
34.
Modulation
This modulation caneither inhibit or facilitate pain.
Modulation at a Spinal Level
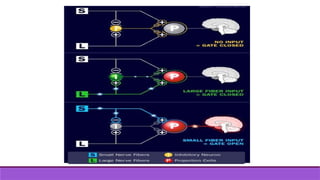
• Without any stimulation, both large and small nerve
fibers are quiet and the inhibitory interneuron (I) blocks
the signal in the projection neuron (P) that connects to
the brain.
• The "gate is closed" and therefore NO PAIN.
35.
• With non-painfulstimulation, large nerve fibers are
activated primarily.
This activates the projection neuron (P), BUT it ALSO
activates the inhibitory interneuron (I) which then
BLOCKS the signal in the projection neuron (P) that
connects to the brain.
The "gate is closed" and therefore NO PAIN.
36.
• With painstimulation, small nerve fibers
become active. They activate the projection neurons
(P) and BLOCK the inhibitory interneuron (I).
Because activity of the inhibitory interneuron is
blocked, it CANNOT block the output of the
projection neuron that connects with the brain.
The "gate is open", therefore, PAIN!!
38.
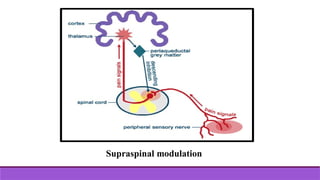
Supraspinal modulation (Descendingmodulation)
Just as there are ascending pain pathways from the body
to the brain, there are also descending pain pathways
communicating from the brain to the body which inhibit
pain.
The most important descending pathways begin in the
periaqueductal gray (PAG).
39.
These descendingpathways are thought to exert their
effect through releasing of serotonin which in turn will
activate the encephalin interneuron located at
substantiagelatinosa.
The released encephalin will act just like the GABA
substance.
Descending Inhibitory Controls
WhileGate Theory Control happens locally (confusing
nerves where the pain happens) another effective
mechanism of pain control is called descending (or
diffuse) noxious inhibitory control, when the pain stimulus
reaches the brain.
42.
The brainsends a signal back to the spinal cord
via a very complex system of nerve
connections: The periaqueductal grey (PAG) in
the midbrain and the rostral ventromedial
medulla (RVM) are two important areas of the
brain involved in descending inhibitory
modulation.
Both these centers contain high concentrations
of opioid receptors and endogenous opioids,
43.
The released opioidssubstances reduce
transmission of the pain impulse that is sent up
to the brain and puts a brake on the pain
impulse as it enters the spinal cord.
Important molecules in this process are endorphin,
enkephalin and serotonin.
Acute vs. ChronicPain
Acute pain
begins suddenly and is usually sharp in quality.
It serves as a warning of disease or a threat to the
body. Acute pain might be mild and last just a
moment, or it might be severe and last for weeks or
months.
47.
In mostcases, acute pain does not last longer than six
months, and it disappears when the underlying cause
of
pain has been treated or has healed.
Unrelieved acute pain, however, might lead to chronic
pain.
48.
Chronic pain
persists despitethe fact that the injury has healed.
Pain signals remain active in the nervous system for
weeks, months, or years. Emotional effects include
depression, anger, anxiety, and fear of re-injury.
Such a fear might hinder a person‘s ability to return
to normal work or leisure activities.
50.
Nociceptive pain vsneuropathic pain
Nociceptive pain
is divided into somatic and visceral. Nociceptive pain
is detected by specialized transducers attached to A-
delta and C fibers.
Somatic pain results from irritation or damage to the
musculoskeletal system. Visceral pain is diffuse,
poorly localized, and often referred.
51.
Neuropathic pain
is paincaused by damage or disease that affects the
somatosensory system. It may be associated with
abnormal sensations called dysesthesia, and pain
produced by normally non-painful stimuli (allodynia).
Neuropathic pain may have continuous and/or episodic
(paroxysmal) components