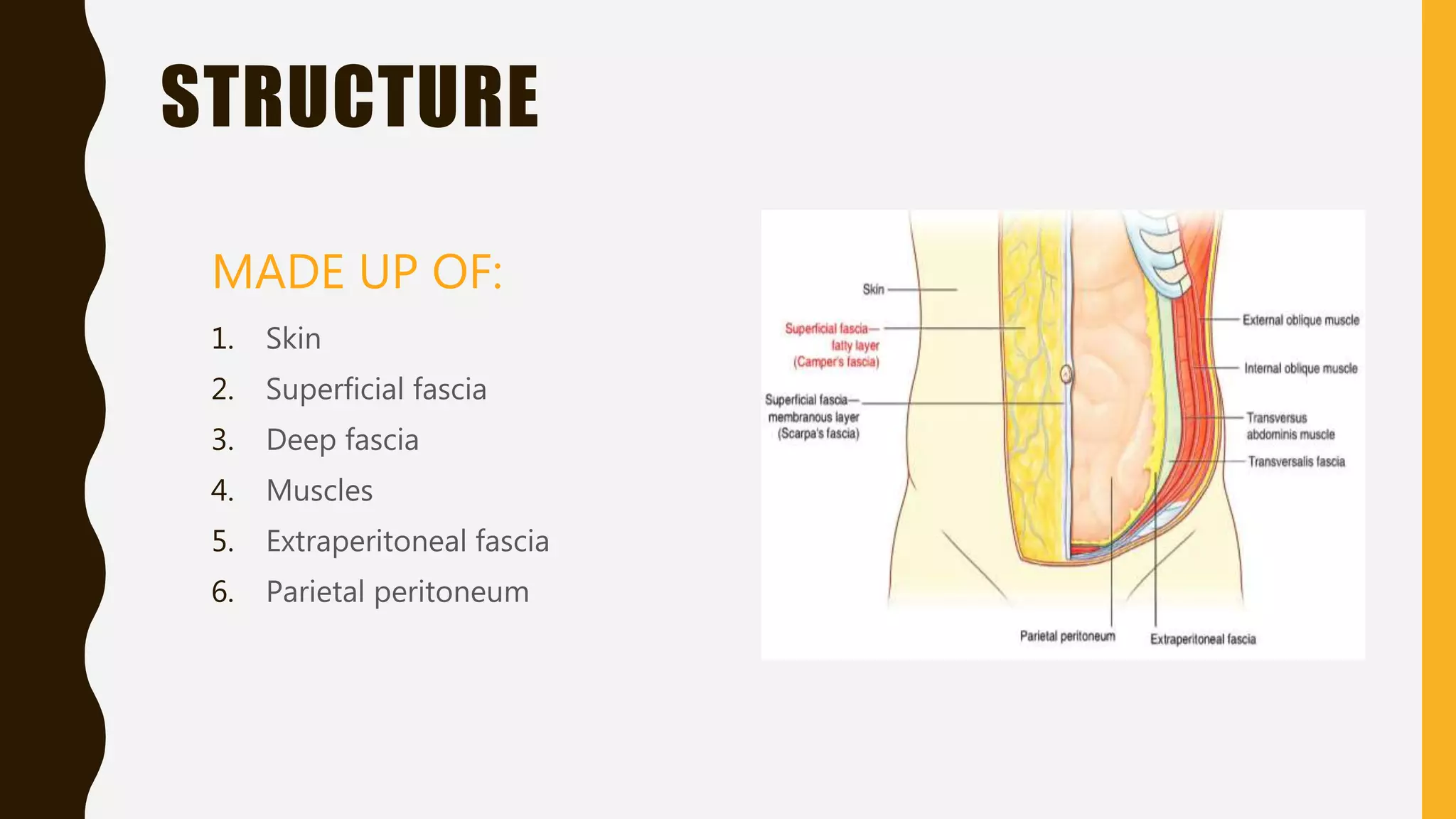
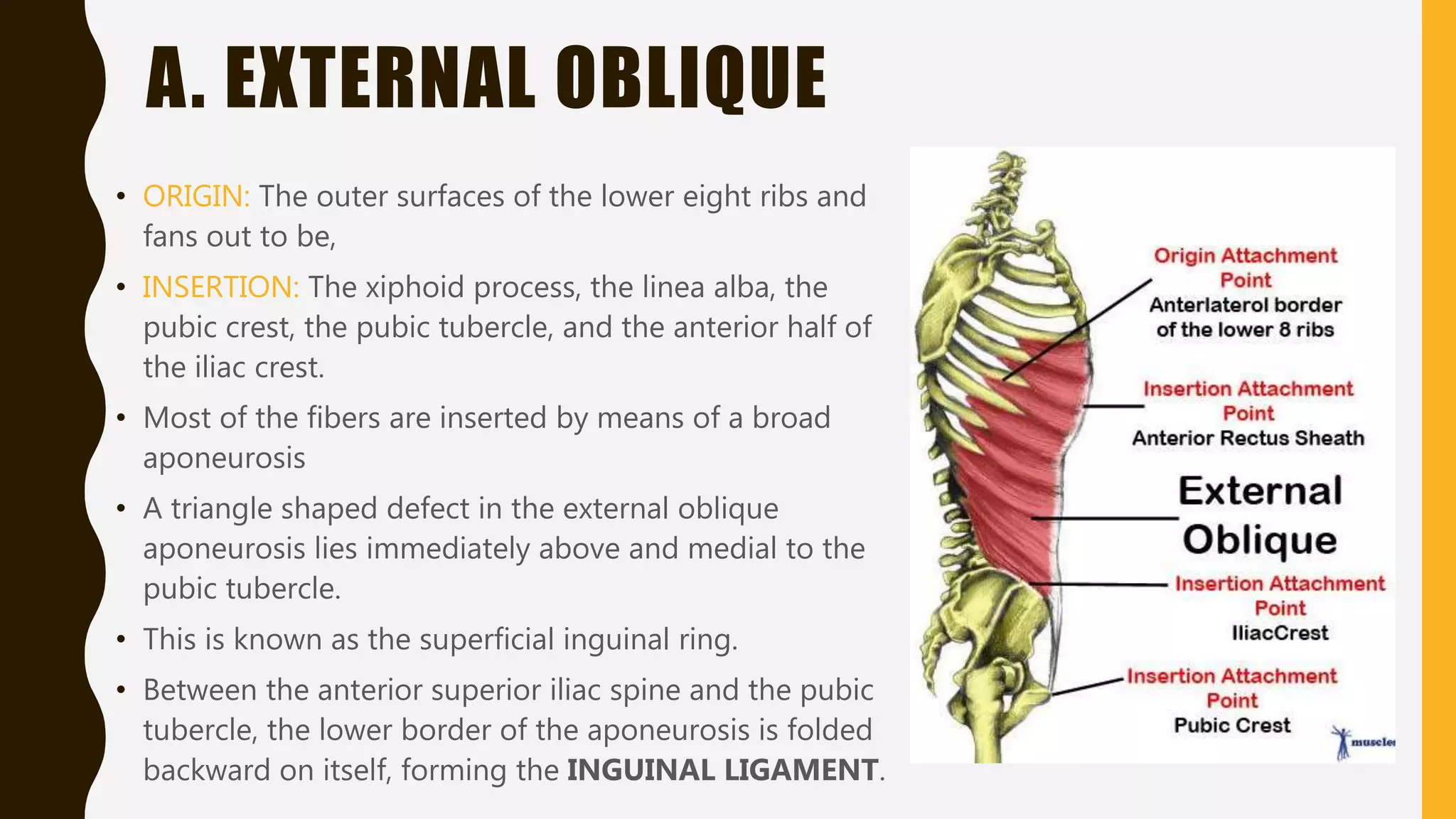
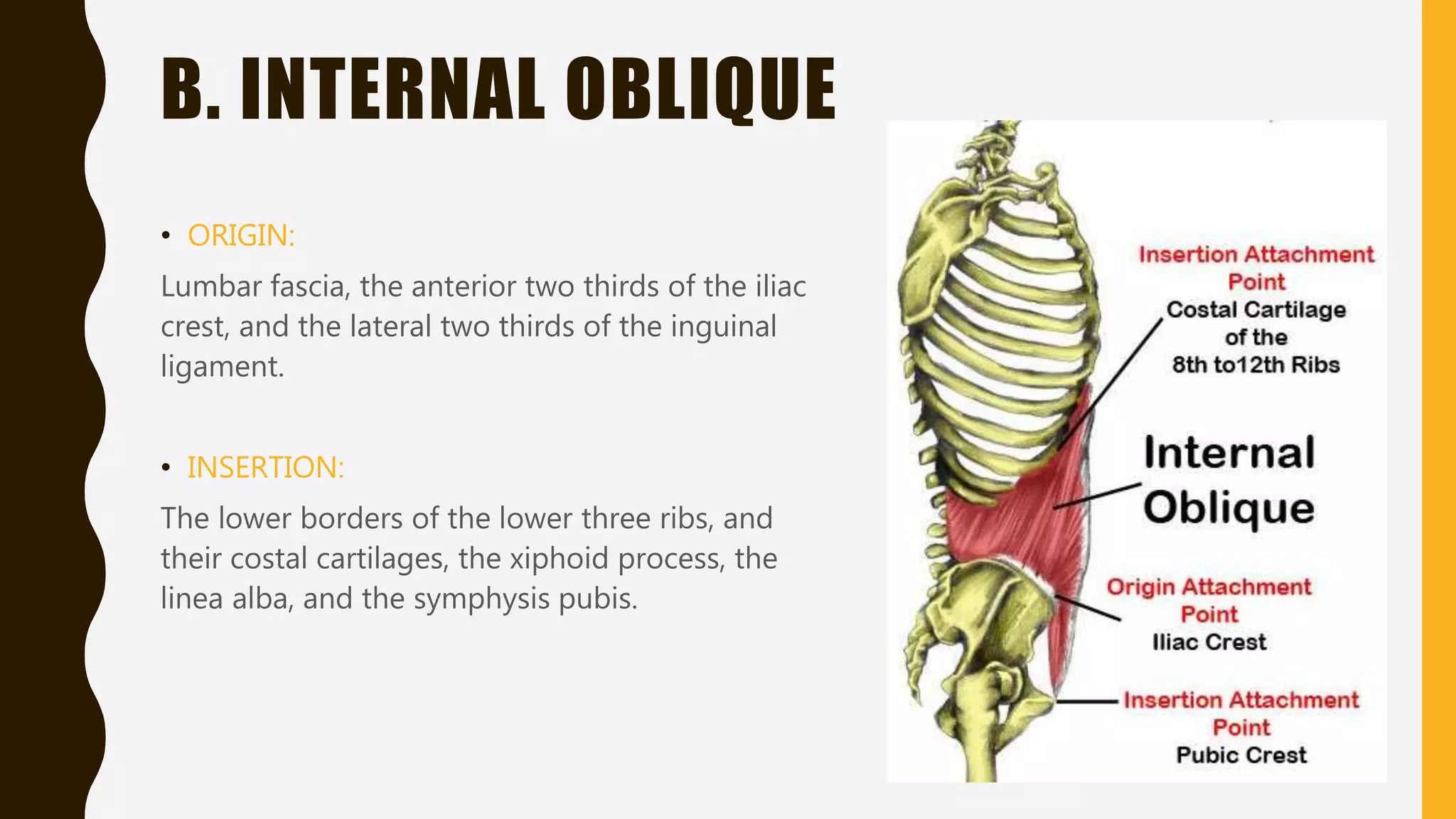
The anterior abdominal wall is made up of skin, superficial fascia, deep fascia, muscles, extraperitoneal fascia, and parietal peritoneum. The major muscles are the external oblique, internal oblique, transversus abdominis, and rectus abdominis. Together, the muscles provide support, protection, and enable functions like micturition, defecation, vomiting, and parturition by increasing intra-abdominal pressure when contracting simultaneously with the diaphragm. The wall receives nerve innervation from the lower thoracic and upper lumbar nerves and has blood supply from branches of the internal mammary, external iliac, and descending thoracic arteries.