Downloaded 40 times


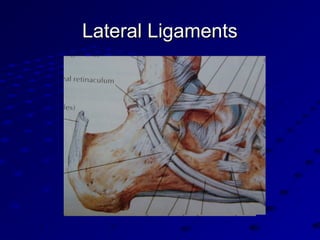









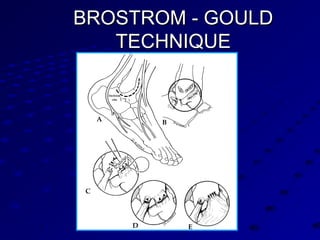
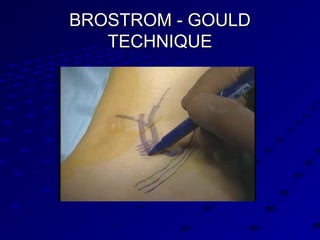

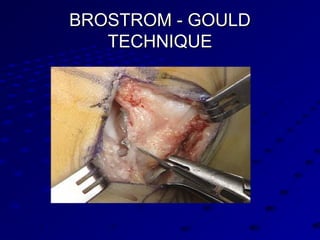








Dr. Girish Motwani is a consultant foot and ankle surgeon with extensive qualifications focusing on both pediatric and adult orthopedics. He emphasizes the prevalence and diagnosis of acute lateral ankle sprains, detailing treatment options, rehabilitation, and indications for surgical intervention. The document concludes by discussing various ankle injuries, their assessment, and the effectiveness of the Brostrom-Gould technique for lateral ligament reconstruction.












































































