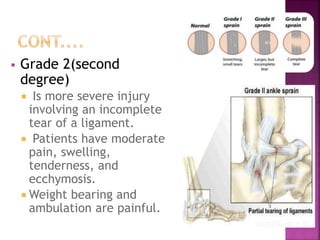
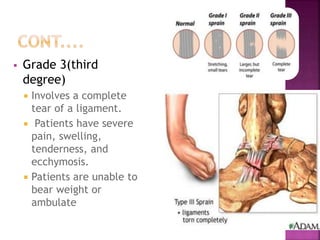
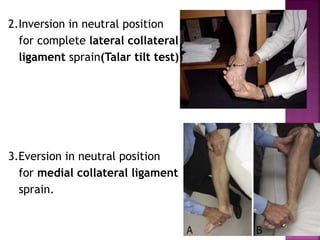
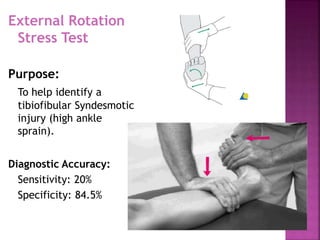
Ankle sprains are ligament injuries, usually caused by forced inversion or plantar flexion of the ankle. Symptoms include pain, swelling, bruising, and difficulty walking. Ankle sprains are classified by severity from Grade 1 (mild stretching) to Grade 3 (complete ligament tear). Physical exams involve stress tests to check for laxity in the anterior talofibular and other ligaments. Conservative treatment focuses on RICE (rest, ice, compression, and elevation) along with rehabilitation exercises. Surgery may be needed for complete tears or chronic instability.






























































![Unidad 3[1][1]](https://cdn.slidesharecdn.com/ss_thumbnails/unidad311-120320081426-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)



















































