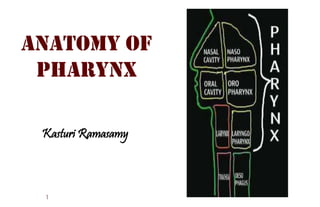
The pharynx is a hollow tube that starts behind the nose, goes down the neck, and ends at the top of the trachea and esophagus. The three parts of the pharynx are the nasopharynx, oropharynx, and hypopharynx.
The pharynx is a hollow tube that starts behind the nose, goes down the neck, and ends at the top of the trachea and esophagus. The three parts of the pharynx are the nasopharynx, oropharynx, and hypopharynx.
The larynx houses the vocal cords, and manipulates pitch and volume, which is essential for phonation. It is situated just below where the tract of the pharynx splits into the trachea and the esophagus.
The parotid gland is a major salivary gland in many animals. In humans, the two parotid glands are present on either side of the mouth and in front of both ears. They are the largest of the salivary glands.
The larynx houses the vocal cords, and manipulates pitch and volume, which is essential for phonation. It is situated just below where the tract of the pharynx splits into the trachea and the esophagus.
The parotid gland is a major salivary gland in many animals. In humans, the two parotid glands are present on either side of the mouth and in front of both ears. They are the largest of the salivary glands.
Daily agri report by epic research limited of 07 march 2017Epic Research
Epic Research Limited consists team of proficient market experts. We offer daily reports on market to facilitate traders gain a quick overview on market's performance .
Pharynx is upper part of the aerodigestive tract. It has three parts nasopharynx, oropharynx and laryngopharynx. Pharynx plays an important part in respiration and swallowing. Swallowing is a very complex process. To swallow properly it is important to shut down the openings of nasopharynx, oral cavity and larynx and open the upper sphinctor of esophagus.
In this seminar we will learn about the development or tongue and oropharynx starting with Pharynx, its Boundaries and Parts, Structure, layers, muscles of pharynx. Then cover the Blood supply, nerve supply and Lymphatic drainage pharynx.
We will also read about Oropharynx and its Relations,
Waldeyer’s lymphatic ring and Physiology of deglutition
Tongue, its Parts, External features and Papillae of the tongue
Muscles of the tongue, Blood supply of the tongue , Arterial and nerve supply, Venous and lymphatic drainage. Development of the tongue and Physiology of taste sensation
Developmental disturbances of the tongue and Periodontal implications are other parts of this seminar
Pulmonary Thromboembolism - etilogy, types, medical- Surgical and nursing man...VarunMahajani
Disruption of blood supply to lung alveoli due to blockage of one or more pulmonary blood vessels is called as Pulmonary thromboembolism. In this presentation we will discuss its causes, types and its management in depth.
Ethanol (CH3CH2OH), or beverage alcohol, is a two-carbon alcohol
that is rapidly distributed in the body and brain. Ethanol alters many
neurochemical systems and has rewarding and addictive properties. It
is the oldest recreational drug and likely contributes to more morbidity,
mortality, and public health costs than all illicit drugs combined. The
5th edition of the Diagnostic and Statistical Manual of Mental Disorders
(DSM-5) integrates alcohol abuse and alcohol dependence into a single
disorder called alcohol use disorder (AUD), with mild, moderate,
and severe subclassifications (American Psychiatric Association, 2013).
In the DSM-5, all types of substance abuse and dependence have been
combined into a single substance use disorder (SUD) on a continuum
from mild to severe. A diagnosis of AUD requires that at least two of
the 11 DSM-5 behaviors be present within a 12-month period (mild
AUD: 2–3 criteria; moderate AUD: 4–5 criteria; severe AUD: 6–11 criteria).
The four main behavioral effects of AUD are impaired control over
drinking, negative social consequences, risky use, and altered physiological
effects (tolerance, withdrawal). This chapter presents an overview
of the prevalence and harmful consequences of AUD in the U.S.,
the systemic nature of the disease, neurocircuitry and stages of AUD,
comorbidities, fetal alcohol spectrum disorders, genetic risk factors, and
pharmacotherapies for AUD.
Explore natural remedies for syphilis treatment in Singapore. Discover alternative therapies, herbal remedies, and lifestyle changes that may complement conventional treatments. Learn about holistic approaches to managing syphilis symptoms and supporting overall health.
Anti ulcer drugs and their Advance pharmacology ||
Anti-ulcer drugs are medications used to prevent and treat ulcers in the stomach and upper part of the small intestine (duodenal ulcers). These ulcers are often caused by an imbalance between stomach acid and the mucosal lining, which protects the stomach lining.
||Scope: Overview of various classes of anti-ulcer drugs, their mechanisms of action, indications, side effects, and clinical considerations.
Ozempic: Preoperative Management of Patients on GLP-1 Receptor Agonists Saeid Safari
Preoperative Management of Patients on GLP-1 Receptor Agonists like Ozempic and Semiglutide
ASA GUIDELINE
NYSORA Guideline
2 Case Reports of Gastric Ultrasound
MANAGEMENT OF ATRIOVENTRICULAR CONDUCTION BLOCK.pdfJim Jacob Roy
Cardiac conduction defects can occur due to various causes.
Atrioventricular conduction blocks ( AV blocks ) are classified into 3 types.
This document describes the acute management of AV block.
Lung Cancer: Artificial Intelligence, Synergetics, Complex System Analysis, S...Oleg Kshivets
RESULTS: Overall life span (LS) was 2252.1±1742.5 days and cumulative 5-year survival (5YS) reached 73.2%, 10 years – 64.8%, 20 years – 42.5%. 513 LCP lived more than 5 years (LS=3124.6±1525.6 days), 148 LCP – more than 10 years (LS=5054.4±1504.1 days).199 LCP died because of LC (LS=562.7±374.5 days). 5YS of LCP after bi/lobectomies was significantly superior in comparison with LCP after pneumonectomies (78.1% vs.63.7%, P=0.00001 by log-rank test). AT significantly improved 5YS (66.3% vs. 34.8%) (P=0.00000 by log-rank test) only for LCP with N1-2. Cox modeling displayed that 5YS of LCP significantly depended on: phase transition (PT) early-invasive LC in terms of synergetics, PT N0—N12, cell ratio factors (ratio between cancer cells- CC and blood cells subpopulations), G1-3, histology, glucose, AT, blood cell circuit, prothrombin index, heparin tolerance, recalcification time (P=0.000-0.038). Neural networks, genetic algorithm selection and bootstrap simulation revealed relationships between 5YS and PT early-invasive LC (rank=1), PT N0—N12 (rank=2), thrombocytes/CC (3), erythrocytes/CC (4), eosinophils/CC (5), healthy cells/CC (6), lymphocytes/CC (7), segmented neutrophils/CC (8), stick neutrophils/CC (9), monocytes/CC (10); leucocytes/CC (11). Correct prediction of 5YS was 100% by neural networks computing (area under ROC curve=1.0; error=0.0).
CONCLUSIONS: 5YS of LCP after radical procedures significantly depended on: 1) PT early-invasive cancer; 2) PT N0--N12; 3) cell ratio factors; 4) blood cell circuit; 5) biochemical factors; 6) hemostasis system; 7) AT; 8) LC characteristics; 9) LC cell dynamics; 10) surgery type: lobectomy/pneumonectomy; 11) anthropometric data. Optimal diagnosis and treatment strategies for LC are: 1) screening and early detection of LC; 2) availability of experienced thoracic surgeons because of complexity of radical procedures; 3) aggressive en block surgery and adequate lymph node dissection for completeness; 4) precise prediction; 5) adjuvant chemoimmunoradiotherapy for LCP with unfavorable prognosis.
- Video recording of this lecture in English language: https://youtu.be/lK81BzxMqdo
- Video recording of this lecture in Arabic language: https://youtu.be/Ve4P0COk9OI
- Link to download the book free: https://nephrotube.blogspot.com/p/nephrotube-nephrology-books.html
- Link to NephroTube website: www.NephroTube.com
- Link to NephroTube social media accounts: https://nephrotube.blogspot.com/p/join-nephrotube-on-social-media.html
New Directions in Targeted Therapeutic Approaches for Older Adults With Mantl...i3 Health
i3 Health is pleased to make the speaker slides from this activity available for use as a non-accredited self-study or teaching resource.
This slide deck presented by Dr. Kami Maddocks, Professor-Clinical in the Division of Hematology and
Associate Division Director for Ambulatory Operations
The Ohio State University Comprehensive Cancer Center, will provide insight into new directions in targeted therapeutic approaches for older adults with mantle cell lymphoma.
STATEMENT OF NEED
Mantle cell lymphoma (MCL) is a rare, aggressive B-cell non-Hodgkin lymphoma (NHL) accounting for 5% to 7% of all lymphomas. Its prognosis ranges from indolent disease that does not require treatment for years to very aggressive disease, which is associated with poor survival (Silkenstedt et al, 2021). Typically, MCL is diagnosed at advanced stage and in older patients who cannot tolerate intensive therapy (NCCN, 2022). Although recent advances have slightly increased remission rates, recurrence and relapse remain very common, leading to a median overall survival between 3 and 6 years (LLS, 2021). Though there are several effective options, progress is still needed towards establishing an accepted frontline approach for MCL (Castellino et al, 2022). Treatment selection and management of MCL are complicated by the heterogeneity of prognosis, advanced age and comorbidities of patients, and lack of an established standard approach for treatment, making it vital that clinicians be familiar with the latest research and advances in this area. In this activity chaired by Michael Wang, MD, Professor in the Department of Lymphoma & Myeloma at MD Anderson Cancer Center, expert faculty will discuss prognostic factors informing treatment, the promising results of recent trials in new therapeutic approaches, and the implications of treatment resistance in therapeutic selection for MCL.
Target Audience
Hematology/oncology fellows, attending faculty, and other health care professionals involved in the treatment of patients with mantle cell lymphoma (MCL).
Learning Objectives
1.) Identify clinical and biological prognostic factors that can guide treatment decision making for older adults with MCL
2.) Evaluate emerging data on targeted therapeutic approaches for treatment-naive and relapsed/refractory MCL and their applicability to older adults
3.) Assess mechanisms of resistance to targeted therapies for MCL and their implications for treatment selection
Tom Selleck Health: A Comprehensive Look at the Iconic Actor’s Wellness Journeygreendigital
Tom Selleck, an enduring figure in Hollywood. has captivated audiences for decades with his rugged charm, iconic moustache. and memorable roles in television and film. From his breakout role as Thomas Magnum in Magnum P.I. to his current portrayal of Frank Reagan in Blue Bloods. Selleck's career has spanned over 50 years. But beyond his professional achievements. fans have often been curious about Tom Selleck Health. especially as he has aged in the public eye.
Follow us on: Pinterest
Introduction
Many have been interested in Tom Selleck health. not only because of his enduring presence on screen but also because of the challenges. and lifestyle choices he has faced and made over the years. This article delves into the various aspects of Tom Selleck health. exploring his fitness regimen, diet, mental health. and the challenges he has encountered as he ages. We'll look at how he maintains his well-being. the health issues he has faced, and his approach to ageing .
Early Life and Career
Childhood and Athletic Beginnings
Tom Selleck was born on January 29, 1945, in Detroit, Michigan, and grew up in Sherman Oaks, California. From an early age, he was involved in sports, particularly basketball. which played a significant role in his physical development. His athletic pursuits continued into college. where he attended the University of Southern California (USC) on a basketball scholarship. This early involvement in sports laid a strong foundation for his physical health and disciplined lifestyle.
Transition to Acting
Selleck's transition from an athlete to an actor came with its physical demands. His first significant role in "Magnum P.I." required him to perform various stunts and maintain a fit appearance. This role, which he played from 1980 to 1988. necessitated a rigorous fitness routine to meet the show's demands. setting the stage for his long-term commitment to health and wellness.
Fitness Regimen
Workout Routine
Tom Selleck health and fitness regimen has evolved. adapting to his changing roles and age. During his "Magnum, P.I." days. Selleck's workouts were intense and focused on building and maintaining muscle mass. His routine included weightlifting, cardiovascular exercises. and specific training for the stunts he performed on the show.
Selleck adjusted his fitness routine as he aged to suit his body's needs. Today, his workouts focus on maintaining flexibility, strength, and cardiovascular health. He incorporates low-impact exercises such as swimming, walking, and light weightlifting. This balanced approach helps him stay fit without putting undue strain on his joints and muscles.
Importance of Flexibility and Mobility
In recent years, Selleck has emphasized the importance of flexibility and mobility in his fitness regimen. Understanding the natural decline in muscle mass and joint flexibility with age. he includes stretching and yoga in his routine. These practices help prevent injuries, improve posture, and maintain mobilit
2. Conical fibromuscular tube –
upper part of the air & food
passages
Location:
Behind the nasal cavity, oral
cavity and larynx
Extend from the base of the
skull to the inferior border of
cricoid cartilage (anteriorly) &
the inferior border of C6
vertebra (posteriorly)
Dimensions:
12-14cm long
Width :
3.5 cm (at its base)
1.5 cm (pharyngo-oesophageal
junction –narrowest part)
2
4. Superior
Base of the skull
• Part of body of
sphenoid
• Basilar part of
occipital bone
Anterior (Incomplete)
Nasal cavity
Oral cavity
Larynx
Posterior
Retropharyngeal
space (between the
buccopharyngeal &
prevertebral fascia)
4
Inferior
Continuous with oesophagus
(at level of C6 & lower border of
circoid cartilage
7. External layer of muscular coat
Constrictor muscles of pharynx
Generally:
Origins are situated
anteriorly
Fibers pass through anterior
& posterior wall of pharynx
All 3 muscles meet in
midline (in a fibrous raphe)
Arrangement:
Inferior constrictor overlaps
the middle constrictor
Middle constrictor overlaps
the superior constrictor
7
8. Superior constrictor muscle
Origin (from above to downwards)
• Pterygoid hamulus
• Pterygomandibular raphe
• Medial surface of mandible at posterior end of mylohyoid line
(near the attachment of pterygomandibular raphe)
• Side of the posterior part of the tongue
8
9. Middle constrictor muscle
Origin
• Lower part of stylohyoid ligament
• Lesser cornu of hyoid bone
• Upper border of greater cornu of hyoid bone
9
10. Inferior constrictor muscle
1. Thyropharnygeus
• Arise from thyroid cartilage
–oblique line and inferior tubercle
of thyroid cartilage
• A tendinous band that crossed
the cricothyroid muscle & is
attached above to the inferior
tubercle of thyroid cartilage
2. Cricopharyngeus
• Cricoid cartilage behind the origin
of cricothyroid muscle
10
11. Internal layer of muscular coat [longitudinal muscles]
1. Stylopharyngeus
From styloid process,
• passes through the gap between superior & middle
constrictor
• Run downward to the inner surface of middle and
inferior constrictor
Stylopharyngeus
muscle
11
12. 2. Palatopharyngeus
• Descends from the sides of palate
• Runs longitudinally on the internal aspect of 3
constrictors
Palatopharyngeus
muscle
12
16. Killian’s Dehiscence
Potential gap between thyropharyngeus with oblique fibers and
the cricopharyngeus with transverse fibers
“Gateway of tears” Perforation can occur at this site during oesophagoscopy
Site for herniation of pharyngeal mucosa in condition of pharyngeal pouch
16
17. Waldeyer’s Ring *inner
• Several aggregations of lymphoid tissue
near the relation of oropharyngeal isthmus
• Composed of:
1. Right & left palatine tonsil (tonsil only)
2. Pharyngeal tonsil (posteriorly & above)
3. Tubal tonsil (laterally & above) –in fossa Rosenmuller
4. Lingual tonsil (posterior part of the dorsum of the
tongue)
5. Palatine tonsils
17
18. Pharyngeal Spaces
1. Retropharyngeal space
• Situated behind the pharynx & extending from the
base of skull to the bifurcation of trachea
• Divided into 2 lateral compartments [spaces of Gillette]
by a fibrous raphe
• Has retropharyngeal nodes –disappear at 3-4
years
• Infection can pass down behind the oesophagus into
the mediastinum
18
19. 2. Parapharyngeal space
• Situated on the side of pharynx
• Contains carotid vessels, jugular vein, last
four cranial nerves & cervical sympathetic
chain
19
20. Parts of pharynx
Laryngopharynx
• Plane of hyoid bone lower border of
cricoid cartilage
20
Nasopharynx
• Base of skull nasopharyngeal isthmus
Oropharynx
• Nasopharyngeal isthmus plane of hyoid
bone
21. Parts of pharynx
1. Nasopharynx
Floor
• Soft palate anteriorly &
is deficient posteriorly
• Oropharynx via
nasopharyngeal
isthmus
Anterior
Nasal cavity via posterior nasal
apertures (choanae)
Lateral
Pharyngeal openings of the eustachian tube
In contact with anterior part of middle ear cavity (opens
at the level of inferior nasal conchae)
Roof
Basisphenoid & Basiocciput
Posterior
Prevertebral muscles &
fascia
21
• Uppermost part of
pharynx (epipharynx)
• Lies behind the
nasal cavity
• Base of skull Soft
palate/Level of the
horizontal plane
passing thru the hard
palate
• Lined by respiratory
epithelium
(pseudostratified
ciliated columnar
epithelium)
• Rigid and non-
collapsible wall
22. Lateral wall of nasopharynx
Pharyngobasillar fascia + Posterior median pharyngeal ligament/raphe
1.25 cm behind the
posterior end of
inferior turbinate
Bounded above
and behind by tubal
elevation (torus
tubarius)
Above and behind
the tubal elevation
is a recess called
fossa of
Rossenmuller
–Lies above the
upper edge of
superior constrictor
muscle & common
site for origin of
carcinoma
• Vertical fold of
mucous
membrane that
is raised by the
salpingopharyn
geus muscle
• Running
downwards from
the posterior
margin of tubal
elevation,
gradually fading
on the side wall
of pharynx
Extend from
anterosuperior
angle of tubal
elevation to soft
palate22
24. Pharyngeal/ Nasopharyngeal
Tonsil/ Adenoids
Sub-epithelial collection of lymphoid tissue at
the junction of roof and posterior wall of
nasopharynx –increases in size up to 6 years
& gradually atrophies.
Tubal tonsil
Collection of sub-epithelial lymphoid tissue
situated at the tubal elevation.
Rathke’s pouch
Dimple above adenoids reminiscent of buccal mucosal
invagination, to form anterior lobe of pituitary.
(*craniopharyngioma may arise from it)
Nasopharyngeal Bursa
• Epithelial lined median recess within adenoid mass &
extends from pharyngeal mucosa to the periosteum of the
basiocciput
• Attachment of notochord to the pharyngeal endoderm
during embryonic life (*abscess –Thornwaldt’s disease)24
25. Sinus of Morgagni
• Space between skull and
upper free border of superior
constrictor muscle.
• Structures passing through this
gap:
Levator veli palatini
Ascending palatine artery
Tensor veli palatini
Eustachian tube
Passavant’s Ridge
• Mucosal ridge raised by fibres of
palatopharyngeus
• Encircles posterior and lateral walls of
nasopharyngeal isthmus
• Soft palate, during its contraction makes
firm contact with this ridge to cut off
nasopharynx from oropharynx during
deglutition or speech
25
26. Lymphatic drainage
• Upper deep cervical nodes through:
Retropharyngeal nodes
Parapharyngeal nodes
• Spinal accessory chain of nodes in the posterior triangle of the
neck
Functions
1. Acts as a conduit for air; nose and
larynx.
2. Ventilates middle ear through
eustachian tube and equalises air
pressure on both sides of TM.
3. Cuts off nasopharynx from
oropharynx with the help of
Passavant’s ridge.
4. Acts as a resonating chamber for
voice production
5. Acts as a drainage channel for
mucus secreted by nasal and
nasopharyngeal glands26
27. Parts of pharynx
2. Oropharynx
Middle part of
the pharynx
behind oral
cavity
Communicates
with:
• Nasopharynx
through
nasopharyngeal
(pharyngeal)
isthmus
• Oral cavity through
the oropharyngeal
isthmus (isthmus of
fauces)
• Laryngopharynx at
the level of upper
border of epiglottis
Lateral wall -Anterior pillar
Palatoglossal arch Lateral wall -
Posterior pillar
Palatopharyngeal arch
Posterior wall
Retropharyngeal space
Opposite to C2 and upper C3 vertebrae
Anterior wall
• Deficient above (communicates
with oral cavity)
• Below:
1. Base of the tongue –posterior
to circumvallate papilla
2. Lingual tonsil
3. Valleculae –cup shaped
depressions lying between the
base of the tongue & anterior
surface of epiglottis
27
“Isthmus of fauces = limit between the mouth cavity proper with the pharynx
marked by constricted aperture Palatopharyngeal and palatoglossal arches”
28. Anterior wall of oropharynx
• Deficient above
(communicates with oral
cavity)
• Below:
1. Base of the tongue –
posterior to circumvallate
papilla
2. Lingual tonsil
3. Valleculae –cup shaped
depressions lying
between the base of the
tongue & anterior surface
of epiglottis
28
30. Lateral wall of oropharynx
Pharyngeal wall
• Forms the lateral
boundaries of tonsillar
fossa
• Composed of (from within
to outward):
1. Pharyngobasilar fascia
2. Superior constrictor &
palatopharyngeus
muscles
3. Buccopharyngeal fascia
4. Styloglossus muscle &
glossopharyngeal nerve
(lower part)
30
32. Lymphatic drainage
• Upper jugular chain: jugulo-digastric nodes (tonsillar)
• Soft palate, lateral & posterior pharyngeal walls & base of
the tongue Retropharyngeal and parapharyngeal
nodes jugulo-digastric & posterior cervical group
Functions
1. Conduit passage for air and food
2. Helps in pharyngeal phase of
deglutition
3. Forms part of vocal tract for speech
sounds
4. Helps in appreciation of taste (taste
buds)
5. Provide local immunity and defense
against harmful intruders
32
33. Parts of pharynx
3. Laryngopharynx (Hypopharynx)
• Lowest part
• Situated behind the larynx
• Extend from upper border of epiglottis to lower
border of cricoid cartilage
Mucosa membrane covering
the lamina of cricoid cartilage
Anterior (Post-cricoid region)
• Laryngeal inlet
• Posterior surface of cricoid and arytenoid cartilage
*common site for carcinoma in females with Plummer Vinson
syndrome
33
34. 34
Lateral wall
[Piriform fossa]
• On each side of laryngeal inlet
• Pharyngoepiglottic fold upper end
of oesophagus
• Boundaries:
Medially: aryepiglottic fold,
posterolateral surfaces of
aryteniud & circoid
cartilages
Laterally: thyroid cartilage &
thyrohyoid membrane
Covered by mucous membrane.
Beneath the membrane is
internal laryngeal nerve
• Smuggler’s fossa -Foreign bodies
may get lodged here
• Removal of foreign body from the
piriform fossa may damage the nerve
anesthesia to the supraglottic part
Posterior
• Level of hyoid bone to the
level of cricoarytenoid joint
35. Lymphatic drainage
• Pyriform sinus upper jugular chain
• Rich lymphatics high frequency of nodal metastasis
in carcinoma of this region
• Post cricoid parapharyngeal LN / nodes of
supraclavicular and paratracheal chain
• Post wall parapharyngeal LN or lateral pharyngeal LN
deep cervical LN
Functions
1. Common pathway for air and food
2. Help in deglutition
3. Provides a vocal tract for resonance of
certain speech sounds
4. Co-ordination between the contraction
of pharyngeal ms and relaxation of
cricopharyngeal sphincter at the upper
end of oesophagus
35
36. Autonomic innervation
Parasympathetic
(secretomotor)
1.Greater petrosal nerve (branch of
facial nerve)
2.Lesser palatine branches of
pterygopalatine ganglion
Sensory innervation
Afferent fibers travel through:
1.Glossopharyngeal nerve (mostly)
2.Vagus nerve (partly)
3.Maxillary nerve through pterygopalatine ganglion (nasopharynx
only)
4.Lesser palatine and glossopharyngeal nerve (soft palate & tonsil)
Motor innervation
• All muscles of pharynx are supplied by the cranial accesory nerve through branches of
vagus except stylopharyngeus muscle[ pharyngeal branches of glossopharyngeal nerve]
• Inferior constrictor muscle has additional supply from the external and recurrent laryngeal nerves
36
Generally, all the nerves supplying the pharynx form a plexus (pharyngeal plexus) which chiefly
lies on the middle constrictor muscle:
1.Pharyngeal branch of vagus carrying cranial accesory nerve fibers
2.Pharyngeal branch of glossopharyngeal nerve
3.Pharyngeal branch of the superior sympathetic ganglion
Fibers from pharyngeal plexus also supplies the muscles of soft palate except tensor veli palatini
(by Mandibular nerve)
37. Blood supply of pharynx
Arterial supply:
1. Ascending pharyngeal branch of
ECA
2. Ascending palatine branch of Facial
artery
3. Tonsillar branch of Facial artery
4. Dorsal lingual branch of lingual artery
5. Greater palatine, pharyngeal branch &
pterygoid branch of maxillary artery
Veins :
Form plexus at the posterolateral aspect
of pharynx, soft palate & prevertebral
region drains into facial and IJV
37