PAROTID GLAND
•
69 likes•9,202 views

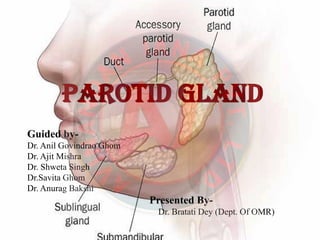
The parotid gland is a major salivary gland in many animals. In humans, the two parotid glands are present on either side of the mouth and in front of both ears. They are the largest of the salivary glands.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to PAROTID GLAND
Similar to PAROTID GLAND (20)
More from Avinandan Jana
More from Avinandan Jana (12)
Recently uploaded
Recently uploaded (20)
PAROTID GLAND
- 1. PAROTID GLANDPAROTID GLAND Guided by- Dr. Anil Govindrao Ghom Dr. Ajit Mishra Dr. Shweta Singh Dr.Savita Ghom Dr. Anurag Bakshi Presented By- Dr. Bratati Dey (Dept. Of OMR)
- 2. CONTENTSCONTENTS Introduction Anatomy of parotid gland Relations Structure with in parotid gland Parotid duct Blood supply Nerve supply Lymphatic drainage Development Parotid lymph node Examination of parotid gland Clinical anatomy References
- 3. IntroductionIntroduction ⁕ Parotid region contains the largest salivary gland and the ““QueenQueen ofof thethe Face”Face” , the facial nerve. ⁕ Para = Around, Otic = ear ⁕ It is the largest salivary gland, situated below the external acquastic meatus.
- 4. Capsule Of Parotid GlandCapsule Of Parotid Gland ⁕ The investing layer of deep cervical fascia forms a capsule for the gland. ⁕ The fascia split (between angle of the mandible and the mastoid process) to enclose gland.
- 5. External featuresExternal features ⁕ The gland resembles a three sided pyramid, apex of the pyramid direct downward ⁕ The gland has four surface and three border.
- 6. Horizontal section of parotid gland showingHorizontal section of parotid gland showing its relation and the structure passingits relation and the structure passing
- 7. Relations of parotid glandRelations of parotid gland The apex overlaps the posterior belly of digastric & the adjoining part of carotid triangle. The cervical branch of facial nerve and the two division of retromandibular vein emerge through it.
- 8. Structure within parotid glandStructure within parotid gland From medial to lateral side these are as follow Arteries ExternalExternal carotidcarotid arteryartery MaxillaryMaxillary arteryartery SuperficialSuperficial temporaltemporal arteryartery It enters the gland through its posteromedial surface It leaves the gland through its antero- medial surface It gives transverse facial artery and emerges at the anterior part of the superior surface.
- 10. Structure within parotid glandStructure within parotid gland Veins – THETHE RETROMANDIBULARRETROMANDIBULAR VEINVEIN is formed within the gland by the union of superficialsuperficial temporaltemporal and maxillarymaxillary veinvein in the lower part of the gland
- 11. Structure within parotid glandStructure within parotid gland Nerve – The FACIALFACIAL NERVENERVE enters the gland through the upper part of its posteromedial surface and divides into 5 terminal branches.
- 12. Facial nerve lies in relation to isthumus of the gland which separate large superficial part from small deep part of the gland.
- 13. PAROTID DUCTPAROTID DUCT Known as STENSEN’S DUCTSTENSEN’S DUCT, 5cm long, carries saliva from gland to oral cavity. It emerges from middle of the anterior border of the gland. It runs forward and slightly downwards on the masseter.
- 14. Superiorly Accessory parotid gland Upper buccal branch of the facial nerve The transverse facial vessels Inferiorly The buccal pad of fat The buccopharyngeal fascia The buccinator
- 15. BLOOD SUPPLYBLOOD SUPPLY TheThe parotidparotid glandgland isis suppliedsupplied byby thethe externalexternal carotidcarotid arteryartery andand itsits branchesbranches thatthat arisesarises withinwithin thethe glandgland.. TheThe veinsveins draindrain intointo externalexternal jugularjugular veinvein andand internalinternal jugularjugular veinvein.. LymphaticLymphatic drainsdrains intointo parotidparotid groupgroup ofof lymphlymph nodenode andand deepdeep cervicalcervical lymphlymph nodenode..
- 17. NERVE SUPPLYNERVE SUPPLY Parasympathetic supply produce watery saliva Pathway-preganglionic fibers begins in inferior salivatory nucleus – 9th nerve – tympanic branch – tympanic plexus – lesserpetrosal nerve –otic ganglion – post ganglionic fibers –auroculo temporal nerve – parotid gland Sympathetic supply produce mucous saliva
- 19. DEVELOPMENTDEVELOPMENT The parotid gland is ectoderm in origin. It developed from the buccal epithelium just lateral to the angle of mouth The outer growth branches form the duct system and acini. The mesoderm form the innerveting connective tissue septa.
- 20. Examination Of Parotid GlandExamination Of Parotid Gland SWELLINGSWELLING- Position of parotid gland. A swelling of parotid gland obliterate the normal hollow just below the lobule of the ear Lymph node swelling are mistaken for parotid gland tumor and vice versa. Note the extend, size, shape and consistency. Whether the swelling is fixed to the masseter muscle or not is confirmed by clinching.
- 21. Examination Of Parotid GlandExamination Of Parotid Gland SKINSKIN OVEROVER PAROTIDPAROTID GLANDGLAND: In case of parotid abscess, edematous skin Fluctuation is very late features of parotid abscess Warm & tender skin Looked for scar & fistula In case of malignancy, check infiltration of the tumor
- 22. Examination Of Parotid GlandExamination Of Parotid Gland DUCTDUCT –– ((stensen’sstensen’s duct)duct) Buccal surface of cheek opposite to upper 2nd molar In case of parotid abscess purulent discharge comes out In malignancy blood will come out Terminal part of duct palpated bidigitally
- 23. Examination Of Parotid GlandExamination Of Parotid Gland EXAMINATION OF FACIAL NERVE- Facial nerve is not involved in benign tumor but involved in malignant growth. LYMPH NODE – Preauricular, parotid, submandibular group of lymph node MOVEMENT OF JAW – Restricted in malignant growth
- 24. CLINICALANATOMYCLINICALANATOMY parotid swelling are very painful due to the underlying nature of the parotid fascia. mumps is an infectious disease of parotid gland caused by paramyxo virus. Viral parotitis or mumps characteristically does not suppurative.
- 25. Developmental abnormalitiesDevelopmental abnormalities AplasiaAplasia oror agenesisagenesis ofof salivarysalivary glandgland – Complete absence of salivary gland is rare but may occur together with other developmental defect. Specially malformation of first & second brancheal arch Agenesis reported along with congenital conditions like Treacher collin syndrome, hemifacial microstomia Also observed in Ectodermal dysplasia
- 26. AccessoryAccessory salivarysalivary DuctsDucts – common, do not require tretment Location- superior and anterior to the normal location of stensen’s duct.
- 27. Diverticula- A diverticula is a pouch or sack protruding from the wall of the duct Diverticula in the duct of major salivary gland often lead to pooling of saliva & recurrent sialadenitis. Diagnosis made by sialography.
- 28. Darier’s Disease- Salivary duct abnormality have been reported in darrier’s disease Also known as dyskeratosis follicularis Diagnosed by sialography
- 29. SialolithiasisSialolithiasis Also known as salivary calculi or salivary stone Etiopathogenesis- NeurohumoralNeurohumoral MechanismMechanism Prevalance- Submandibular 83% Parotid 10% Sublingual 7%
- 31. SialolithiasisSialolithiasis ClinicalClinical featuresfeatures-- Pain, swelling acute suppurative process, pus, ulceration, absence of salivation Swab test RadiographicRadiographic featuresfeatures-- For parotidparotid glandgland periapical view in the buccal vestibule, reduce exposure to avoid burnout sialolith
- 32. SialographySialography Sialography is indicated when sialolith are radiolucent. The film usually shows contrast medium present behind the stone. In some cases ‘cherry‘cherry blossomblossom’ or ‘fruitfruit ladenladen branchlessbranchless treetree’ appearance seen.
- 33. • Contrast media for sialography TYPESTYPES Iodine based Ionic aqueous solution Non ionic aquous solution Oil based Iodized oil (lipiodol)
- 34. FREYFREY SYNDROMESYNDROME- Also known as AuriculoAuriculo TemporalTemporal SyndromeSyndrome Parotidectyomy is the removal of parotid gland. After this operation there may be regeneration of secretomotor fibers in the auriculotempral nerve which join the grater auricular nerve This causes stimulation of the sweet gland → hyperamia → Redness & sweating in the area of skin
- 35. PleomorphicPleomorphic AdenomaAdenoma • The term was suggested by willis characterizing unusual histological pattern. • Also known as- ‘iceberg tumor’, ‘endothelioma’. • Most common benign salivary gland tumor. • Clinical features –small, painless, round to oval lobulated, dumbbells shaped appearance, sometimes erosion of the underlying bone. • Management- surgical excision
- 36. WarthinWarthin TumorTumor [Papillary[Papillary CystadenomaCystadenoma LymphomatosumLymphomatosum]] Benign neoplasm Occurs almost exclusively in the parotid gland 2nd most common benign tumor Clinical features- slow growing, painless, nodular mass, firm on palpation, 6th -7th decade of life Risk factor- smokers
- 37. Mikulicz’sMikulicz’s diseasedisease Synonyms- Benign lympho-epithelial lesions. First described by MikuliczMikulicz in 1888 It is an Autoimmune disorder. Unilateral / bilateral enlargement of parotid gland Prodromal symptoms- fever, URTI, oral infection, tooth extraction. Mild local discomfort, diffuse, poorly outline enlargement of salivary gland Management- surgical excision
- 38. Basal cell adenomaBasal cell adenoma Age/sex- Female > male, older age group Occurs primarily in major salivary gland, particularly in the parotid gland Symptoms- painless, slow growing. Diagnosis- difficult to make clinical diagnosis, Biopsy shown fairly well defined connective tissue capsule the cells are isomorphic and baseloid with round nuclei. T/t- surgical excision, recurrence rate is rare
- 39. MucoepidermoidMucoepidermoid CarcinomaCarcinoma It is a malignant tumor of salivary gland. Malignant tumors comprise 15–32% of parotid tumors, 41– 45% of submandibular tumors and 70–90% of sublingual tumors. It occurs in 2nd-7th decade
- 40. Clinical Staging of salivary glandClinical Staging of salivary gland tumortumor By spiro Staging of salivary gland neoplasm T₁:0-3cm solitary and freely mobile & CRVII intact T₂:3.1-6cm, solitary & freely mobile skin or fixed CRVII intact T₃:6cm or multiple nodules or ulceration or deep fixation or CRVII dysfunction Patient with T₁ & T₂ =stage I & stage II respectively Metastasis of lymphnodes with T₃ lesion = stage III
- 41. By American joint committee Ptimary tumor- Tx: can’t be assessed by rules T₀: no evidence of primary tumor T₁: 0-2cm T₂: 2-4cm, without significant local extension T₃: 4-6cm, without significant local extension T₄ₐ: >6cm without local extension T₄b: any size with significant local extension
- 42. Nodal involvement- Nₓ: can’t be assessed N₀: no regional lymph node metastasis N₁: clinical / histologically positive regional lymph nodes Distant metastasis- Mₓ: distant metastasis can’t be assessed M₀: no distant metastasis M₁: Distant metastasis
- 43. Stage grouping is performed as followStage grouping is performed as follow Stage I Stage II Stage III Stage IV T₁N₀M₀ or T₂N₀M₀ T₃N₀M₀ T₁ or T₂N₀M₀ or T₄ₐ or T₄bN₀M₀ T₃N₁M₀ or T₄ₐ or T₄bN₁M₀ or Any T any N M₁
- 44. Diagnostic test of the salivary glandDiagnostic test of the salivary gland Sialography Scintigraphy USG CT ScanArteriography MRI Flow rate study
- 45. ScintigraphyScintigraphy o Also known as salivary gland scanning. o It is used for studying glandular parenchyma. o The salivary gland tissue take up compound of iodine bromine & technetium oo IndicationIndication- o Salivary gland function o Allow bilateral comparison o Image of all four gland at the same time.
- 46. UltrasonographyUltrasonography It involves transmission of energy into salivary tissue, receiving of the energy after it has been reflected by the tissue & recording it so that it can be presented by the interpretation. Useful for radiolucent stone. Different echo signals are obtained from different tumors.
- 48. CT SCANCT SCAN It demonstrated small differences in soft tissues X-ray examination & distinction between gland & adjacent soft tissue is improved. IndicationIndication Both Intrinsic and Extrinsic swelling
- 50. ArteriographyArteriography It will define the vasculature of the tumor but also delineate the vascular supply.
- 51. MagneticMagnetic Resonance ImagingResonance Imaging Useful in discrete swelling of salivary gland and provide excellent soft tissue details. It readily enables differentiation between the normal and abnormal.
- 52. REFERENCESREFERENCES B D Chaurasia’s HUMAN ANATOMY volume 3, Krishna Garg Fifth edition 141-146 Burket’s ORAL MEDICINE, Michael Glick 12th edition 232-236 Textbook of ORAL MEDICINE Anil Govindrao Ghom, Third edition 42-43 Nicolas Landis, Pleomorphic Adenoma of the Parotid Gland The American Journal of Medicine, Vol 129, No 1, January 2016 Fondazione IRCCS et al, Major and minor salivary gland tumors Critical Reviews in Oncology/Hematology 74 (2010) 134–148 Ravikiran ongole, Praveen B N, Text book of oral medicine oral diagnosis and oral radiology 332-368
- 53. Thank you