The larynx houses the vocal cords, and manipulates pitch and volume, which is essential for phonation. It is situated just below where the tract of the pharynx splits into the trachea and the esophagus.
The larynx houses the vocal cords, and manipulates pitch and volume, which is essential for phonation. It is situated just below where the tract of the pharynx splits into the trachea and the esophagus.
Granulomatous diseases of the larynx- ALL DETAILS ABOUT TB, FUNGAL LARYNGITIS, SARCOIDOSIS, SYPHILIS, LEPROSY, Wegner granulomatosis, rhinoscleroma ARE GIVEN
Granulomatous diseases of the larynx- ALL DETAILS ABOUT TB, FUNGAL LARYNGITIS, SARCOIDOSIS, SYPHILIS, LEPROSY, Wegner granulomatosis, rhinoscleroma ARE GIVEN
The Larynx: Anatomy, Function, and Disorders
Introduction
The larynx, commonly known as the voice box, is a vital structure in the human body responsible for a multitude of functions, the most prominent of which is voice production. This complex organ plays a crucial role in breathing, swallowing, and protecting the airway. Understanding the anatomy, function, and common disorders of the larynx is essential for grasping its significance in our daily lives. In this comprehensive 2000-word essay, we will explore the larynx in detail, delving into its anatomy, function, the mechanics of voice production, common laryngeal disorders, and their treatment.
I. Anatomy of the Larynx
The larynx is a complex structure located in the neck, connecting the lower part of the pharynx to the trachea. It comprises several cartilages, muscles, ligaments, and other anatomical components that work together to facilitate various functions. To understand the larynx better, it is crucial to break down its anatomy into its constituent parts.
Cartilages
A. Thyroid Cartilage: The thyroid cartilage, often referred to as the Adam's apple, is the most prominent and easily palpable cartilage of the larynx. It is made up of two fused plates and provides structural support to the front of the larynx.
B. Cricoid Cartilage: The cricoid cartilage is a ring-like structure that sits just below the thyroid cartilage. It plays a crucial role in connecting the larynx to the trachea and provides structural support.
C. Epiglottis: The epiglottis is a leaf-shaped cartilage located behind the tongue root. It acts as a lid to cover the entrance of the trachea during swallowing, preventing food and liquids from entering the airway.
D. Arytenoid Cartilages: These paired cartilages are located on top of the cricoid cartilage. They play a pivotal role in controlling vocal cord tension and movement.
E. Corniculate and Cuneiform Cartilages: These smaller cartilages are positioned within the aryepiglottic folds and aid in maintaining the laryngeal structure.
Muscles
A. Intrinsic Laryngeal Muscles: These muscles are responsible for controlling the position and tension of the vocal cords. Key intrinsic muscles include the cricothyroid, thyroarytenoid, lateral cricoarytenoid, posterior cricoarytenoid, and interarytenoid muscles.
B. Extrinsic Laryngeal Muscles: Extrinsic muscles are responsible for moving the larynx as a whole, helping with functions such as swallowing and speech. The sternothyroid, thyrohyoid, and omohyoid muscles are examples of extrinsic laryngeal muscles.
Vocal Cords
The vocal cords, or vocal folds, are a pair of muscular structures located within the larynx. They are composed of layers of mucous membrane, muscle, and connective tissue. The true vocal cords, also known as the vocal ligaments, are the structures primarily responsible for sound production. They are capable of opening and closing rapidly to produce sound when air flows through them.
Report Back from SGO 2024: What’s the Latest in Cervical Cancer?bkling
Are you curious about what’s new in cervical cancer research or unsure what the findings mean? Join Dr. Emily Ko, a gynecologic oncologist at Penn Medicine, to learn about the latest updates from the Society of Gynecologic Oncology (SGO) 2024 Annual Meeting on Women’s Cancer. Dr. Ko will discuss what the research presented at the conference means for you and answer your questions about the new developments.
ARTIFICIAL INTELLIGENCE IN HEALTHCARE.pdfAnujkumaranit
Artificial intelligence (AI) refers to the simulation of human intelligence processes by machines, especially computer systems. It encompasses tasks such as learning, reasoning, problem-solving, perception, and language understanding. AI technologies are revolutionizing various fields, from healthcare to finance, by enabling machines to perform tasks that typically require human intelligence.
Pulmonary Thromboembolism - etilogy, types, medical- Surgical and nursing man...VarunMahajani
Disruption of blood supply to lung alveoli due to blockage of one or more pulmonary blood vessels is called as Pulmonary thromboembolism. In this presentation we will discuss its causes, types and its management in depth.
Ethanol (CH3CH2OH), or beverage alcohol, is a two-carbon alcohol
that is rapidly distributed in the body and brain. Ethanol alters many
neurochemical systems and has rewarding and addictive properties. It
is the oldest recreational drug and likely contributes to more morbidity,
mortality, and public health costs than all illicit drugs combined. The
5th edition of the Diagnostic and Statistical Manual of Mental Disorders
(DSM-5) integrates alcohol abuse and alcohol dependence into a single
disorder called alcohol use disorder (AUD), with mild, moderate,
and severe subclassifications (American Psychiatric Association, 2013).
In the DSM-5, all types of substance abuse and dependence have been
combined into a single substance use disorder (SUD) on a continuum
from mild to severe. A diagnosis of AUD requires that at least two of
the 11 DSM-5 behaviors be present within a 12-month period (mild
AUD: 2–3 criteria; moderate AUD: 4–5 criteria; severe AUD: 6–11 criteria).
The four main behavioral effects of AUD are impaired control over
drinking, negative social consequences, risky use, and altered physiological
effects (tolerance, withdrawal). This chapter presents an overview
of the prevalence and harmful consequences of AUD in the U.S.,
the systemic nature of the disease, neurocircuitry and stages of AUD,
comorbidities, fetal alcohol spectrum disorders, genetic risk factors, and
pharmacotherapies for AUD.
NVBDCP.pptx Nation vector borne disease control programSapna Thakur
NVBDCP was launched in 2003-2004 . Vector-Borne Disease: Disease that results from an infection transmitted to humans and other animals by blood-feeding arthropods, such as mosquitoes, ticks, and fleas. Examples of vector-borne diseases include Dengue fever, West Nile Virus, Lyme disease, and malaria.
Flu Vaccine Alert in Bangalore Karnatakaaddon Scans
As flu season approaches, health officials in Bangalore, Karnataka, are urging residents to get their flu vaccinations. The seasonal flu, while common, can lead to severe health complications, particularly for vulnerable populations such as young children, the elderly, and those with underlying health conditions.
Dr. Vidisha Kumari, a leading epidemiologist in Bangalore, emphasizes the importance of getting vaccinated. "The flu vaccine is our best defense against the influenza virus. It not only protects individuals but also helps prevent the spread of the virus in our communities," he says.
This year, the flu season is expected to coincide with a potential increase in other respiratory illnesses. The Karnataka Health Department has launched an awareness campaign highlighting the significance of flu vaccinations. They have set up multiple vaccination centers across Bangalore, making it convenient for residents to receive their shots.
To encourage widespread vaccination, the government is also collaborating with local schools, workplaces, and community centers to facilitate vaccination drives. Special attention is being given to ensuring that the vaccine is accessible to all, including marginalized communities who may have limited access to healthcare.
Residents are reminded that the flu vaccine is safe and effective. Common side effects are mild and may include soreness at the injection site, mild fever, or muscle aches. These side effects are generally short-lived and far less severe than the flu itself.
Healthcare providers are also stressing the importance of continuing COVID-19 precautions. Wearing masks, practicing good hand hygiene, and maintaining social distancing are still crucial, especially in crowded places.
Protect yourself and your loved ones by getting vaccinated. Together, we can help keep Bangalore healthy and safe this flu season. For more information on vaccination centers and schedules, residents can visit the Karnataka Health Department’s official website or follow their social media pages.
Stay informed, stay safe, and get your flu shot today!
Ozempic: Preoperative Management of Patients on GLP-1 Receptor Agonists Saeid Safari
Preoperative Management of Patients on GLP-1 Receptor Agonists like Ozempic and Semiglutide
ASA GUIDELINE
NYSORA Guideline
2 Case Reports of Gastric Ultrasound
- Video recording of this lecture in English language: https://youtu.be/lK81BzxMqdo
- Video recording of this lecture in Arabic language: https://youtu.be/Ve4P0COk9OI
- Link to download the book free: https://nephrotube.blogspot.com/p/nephrotube-nephrology-books.html
- Link to NephroTube website: www.NephroTube.com
- Link to NephroTube social media accounts: https://nephrotube.blogspot.com/p/join-nephrotube-on-social-media.html
Title: Sense of Taste
Presenter: Dr. Faiza, Assistant Professor of Physiology
Qualifications:
MBBS (Best Graduate, AIMC Lahore)
FCPS Physiology
ICMT, CHPE, DHPE (STMU)
MPH (GC University, Faisalabad)
MBA (Virtual University of Pakistan)
Learning Objectives:
Describe the structure and function of taste buds.
Describe the relationship between the taste threshold and taste index of common substances.
Explain the chemical basis and signal transduction of taste perception for each type of primary taste sensation.
Recognize different abnormalities of taste perception and their causes.
Key Topics:
Significance of Taste Sensation:
Differentiation between pleasant and harmful food
Influence on behavior
Selection of food based on metabolic needs
Receptors of Taste:
Taste buds on the tongue
Influence of sense of smell, texture of food, and pain stimulation (e.g., by pepper)
Primary and Secondary Taste Sensations:
Primary taste sensations: Sweet, Sour, Salty, Bitter, Umami
Chemical basis and signal transduction mechanisms for each taste
Taste Threshold and Index:
Taste threshold values for Sweet (sucrose), Salty (NaCl), Sour (HCl), and Bitter (Quinine)
Taste index relationship: Inversely proportional to taste threshold
Taste Blindness:
Inability to taste certain substances, particularly thiourea compounds
Example: Phenylthiocarbamide
Structure and Function of Taste Buds:
Composition: Epithelial cells, Sustentacular/Supporting cells, Taste cells, Basal cells
Features: Taste pores, Taste hairs/microvilli, and Taste nerve fibers
Location of Taste Buds:
Found in papillae of the tongue (Fungiform, Circumvallate, Foliate)
Also present on the palate, tonsillar pillars, epiglottis, and proximal esophagus
Mechanism of Taste Stimulation:
Interaction of taste substances with receptors on microvilli
Signal transduction pathways for Umami, Sweet, Bitter, Sour, and Salty tastes
Taste Sensitivity and Adaptation:
Decrease in sensitivity with age
Rapid adaptation of taste sensation
Role of Saliva in Taste:
Dissolution of tastants to reach receptors
Washing away the stimulus
Taste Preferences and Aversions:
Mechanisms behind taste preference and aversion
Influence of receptors and neural pathways
Impact of Sensory Nerve Damage:
Degeneration of taste buds if the sensory nerve fiber is cut
Abnormalities of Taste Detection:
Conditions: Ageusia, Hypogeusia, Dysgeusia (parageusia)
Causes: Nerve damage, neurological disorders, infections, poor oral hygiene, adverse drug effects, deficiencies, aging, tobacco use, altered neurotransmitter levels
Neurotransmitters and Taste Threshold:
Effects of serotonin (5-HT) and norepinephrine (NE) on taste sensitivity
Supertasters:
25% of the population with heightened sensitivity to taste, especially bitterness
Increased number of fungiform papillae
These lecture slides, by Dr Sidra Arshad, offer a quick overview of physiological basis of a normal electrocardiogram.
Learning objectives:
1. Define an electrocardiogram (ECG) and electrocardiography
2. Describe how dipoles generated by the heart produce the waveforms of the ECG
3. Describe the components of a normal electrocardiogram of a typical bipolar leads (limb II)
4. Differentiate between intervals and segments
5. Enlist some common indications for obtaining an ECG
Study Resources:
1. Chapter 11, Guyton and Hall Textbook of Medical Physiology, 14th edition
2. Chapter 9, Human Physiology - From Cells to Systems, Lauralee Sherwood, 9th edition
3. Chapter 29, Ganong’s Review of Medical Physiology, 26th edition
4. Electrocardiogram, StatPearls - https://www.ncbi.nlm.nih.gov/books/NBK549803/
5. ECG in Medical Practice by ABM Abdullah, 4th edition
6. ECG Basics, http://www.nataliescasebook.com/tag/e-c-g-basics
Title: Sense of Smell
Presenter: Dr. Faiza, Assistant Professor of Physiology
Qualifications:
MBBS (Best Graduate, AIMC Lahore)
FCPS Physiology
ICMT, CHPE, DHPE (STMU)
MPH (GC University, Faisalabad)
MBA (Virtual University of Pakistan)
Learning Objectives:
Describe the primary categories of smells and the concept of odor blindness.
Explain the structure and location of the olfactory membrane and mucosa, including the types and roles of cells involved in olfaction.
Describe the pathway and mechanisms of olfactory signal transmission from the olfactory receptors to the brain.
Illustrate the biochemical cascade triggered by odorant binding to olfactory receptors, including the role of G-proteins and second messengers in generating an action potential.
Identify different types of olfactory disorders such as anosmia, hyposmia, hyperosmia, and dysosmia, including their potential causes.
Key Topics:
Olfactory Genes:
3% of the human genome accounts for olfactory genes.
400 genes for odorant receptors.
Olfactory Membrane:
Located in the superior part of the nasal cavity.
Medially: Folds downward along the superior septum.
Laterally: Folds over the superior turbinate and upper surface of the middle turbinate.
Total surface area: 5-10 square centimeters.
Olfactory Mucosa:
Olfactory Cells: Bipolar nerve cells derived from the CNS (100 million), with 4-25 olfactory cilia per cell.
Sustentacular Cells: Produce mucus and maintain ionic and molecular environment.
Basal Cells: Replace worn-out olfactory cells with an average lifespan of 1-2 months.
Bowman’s Gland: Secretes mucus.
Stimulation of Olfactory Cells:
Odorant dissolves in mucus and attaches to receptors on olfactory cilia.
Involves a cascade effect through G-proteins and second messengers, leading to depolarization and action potential generation in the olfactory nerve.
Quality of a Good Odorant:
Small (3-20 Carbon atoms), volatile, water-soluble, and lipid-soluble.
Facilitated by odorant-binding proteins in mucus.
Membrane Potential and Action Potential:
Resting membrane potential: -55mV.
Action potential frequency in the olfactory nerve increases with odorant strength.
Adaptation Towards the Sense of Smell:
Rapid adaptation within the first second, with further slow adaptation.
Psychological adaptation greater than receptor adaptation, involving feedback inhibition from the central nervous system.
Primary Sensations of Smell:
Camphoraceous, Musky, Floral, Pepperminty, Ethereal, Pungent, Putrid.
Odor Detection Threshold:
Examples: Hydrogen sulfide (0.0005 ppm), Methyl-mercaptan (0.002 ppm).
Some toxic substances are odorless at lethal concentrations.
Characteristics of Smell:
Odor blindness for single substances due to lack of appropriate receptor protein.
Behavioral and emotional influences of smell.
Transmission of Olfactory Signals:
From olfactory cells to glomeruli in the olfactory bulb, involving lateral inhibition.
Primitive, less old, and new olfactory systems with different path
The prostate is an exocrine gland of the male mammalian reproductive system
It is a walnut-sized gland that forms part of the male reproductive system and is located in front of the rectum and just below the urinary bladder
Function is to store and secrete a clear, slightly alkaline fluid that constitutes 10-30% of the volume of the seminal fluid that along with the spermatozoa, constitutes semen
A healthy human prostate measures (4cm-vertical, by 3cm-horizontal, 2cm ant-post ).
It surrounds the urethra just below the urinary bladder. It has anterior, median, posterior and two lateral lobes
It’s work is regulated by androgens which are responsible for male sex characteristics
Generalised disease of the prostate due to hormonal derangement which leads to non malignant enlargement of the gland (increase in the number of epithelial cells and stromal tissue)to cause compression of the urethra leading to symptoms (LUTS
Lung Cancer: Artificial Intelligence, Synergetics, Complex System Analysis, S...Oleg Kshivets
RESULTS: Overall life span (LS) was 2252.1±1742.5 days and cumulative 5-year survival (5YS) reached 73.2%, 10 years – 64.8%, 20 years – 42.5%. 513 LCP lived more than 5 years (LS=3124.6±1525.6 days), 148 LCP – more than 10 years (LS=5054.4±1504.1 days).199 LCP died because of LC (LS=562.7±374.5 days). 5YS of LCP after bi/lobectomies was significantly superior in comparison with LCP after pneumonectomies (78.1% vs.63.7%, P=0.00001 by log-rank test). AT significantly improved 5YS (66.3% vs. 34.8%) (P=0.00000 by log-rank test) only for LCP with N1-2. Cox modeling displayed that 5YS of LCP significantly depended on: phase transition (PT) early-invasive LC in terms of synergetics, PT N0—N12, cell ratio factors (ratio between cancer cells- CC and blood cells subpopulations), G1-3, histology, glucose, AT, blood cell circuit, prothrombin index, heparin tolerance, recalcification time (P=0.000-0.038). Neural networks, genetic algorithm selection and bootstrap simulation revealed relationships between 5YS and PT early-invasive LC (rank=1), PT N0—N12 (rank=2), thrombocytes/CC (3), erythrocytes/CC (4), eosinophils/CC (5), healthy cells/CC (6), lymphocytes/CC (7), segmented neutrophils/CC (8), stick neutrophils/CC (9), monocytes/CC (10); leucocytes/CC (11). Correct prediction of 5YS was 100% by neural networks computing (area under ROC curve=1.0; error=0.0).
CONCLUSIONS: 5YS of LCP after radical procedures significantly depended on: 1) PT early-invasive cancer; 2) PT N0--N12; 3) cell ratio factors; 4) blood cell circuit; 5) biochemical factors; 6) hemostasis system; 7) AT; 8) LC characteristics; 9) LC cell dynamics; 10) surgery type: lobectomy/pneumonectomy; 11) anthropometric data. Optimal diagnosis and treatment strategies for LC are: 1) screening and early detection of LC; 2) availability of experienced thoracic surgeons because of complexity of radical procedures; 3) aggressive en block surgery and adequate lymph node dissection for completeness; 4) precise prediction; 5) adjuvant chemoimmunoradiotherapy for LCP with unfavorable prognosis.
micro teaching on communication m.sc nursing.pdfAnurag Sharma
Microteaching is a unique model of practice teaching. It is a viable instrument for the. desired change in the teaching behavior or the behavior potential which, in specified types of real. classroom situations, tends to facilitate the achievement of specified types of objectives.
2. OBJECTIVES
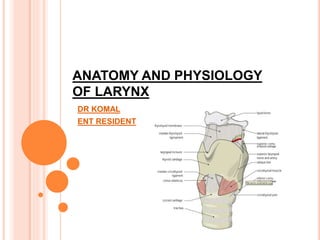
•To discuss the basic anatomy of the larynx
•To enumerate the main functions of the
larynx
3. LARYNX:
Commonly called- voice box
Shape- tube shaped.
Composed- muscles, cartilages, connective
tissue.
Location- in front of hypopharynx 3-6 cervical vertebra.
Moves vertically in AP direction and can be passively moved
from side to side producing grating sensation called
Larnyngeal crepitus.
4.
5.
6. SHAPE AND SIZE:
the shape of the larynx in lower side is circular and
from the upper it is triangular in shape.
Its length is 4.3 cm
transverse diameter is 4.2 cm and anterior
posterior diameter 3.6 cm.
8. THYROID CARTILAGE:
Largest cartilage consist of two alae meets anteriorly forming
an angle of 90 in males and 120 in females.
Vc are attached to the middle of thyroid angle.
Most of the laryngeal fb are arrested above the vc.
larger in males than females
Hyaline cartilage
9. LINNING OF THE LARYNX:
superior of the vocal fold is non karatinized
stratified squamous epithelium,
inferior to the vocal fold is pseudo stratified
columnar epithelium.
10. posterior angles are prolonged into processes
termed as the superior and inferior cornu.
The superior cornu is long, and narrow, directed
upward, backward,and Medially which gives
attachment to the lateral hypothyroid ligament.
•The inferior cornu is short and thick, it is directed
downward.
11. CRICOID CARTILAGE:
A ring of hyaline cartilage known as SIGNET RING.
Hyaline cartilage.
It is the only cartilage that forms a complete ring..
Its post part is expanded to form a Lamina while anteriorly it
forms an arch. it forms the lower and posterior parts of the
wall of the larynx.
attached to the first ring of cartilage of the trachea by the
cricotracheal ligament
the thyroid cartilage is connected to the cricoid cartilage by the
cricothyroid ligament.
12.
13. EPIGLOTTIS:
•It is a large leaf-shaped piece of elastic cartilage, it forms
anterior wall of laryngeal inlet.
It is attached to the body of hyoid bone by hypoepiglottic
ligament, which divides it into the suprahyoid and infrahyoid
epiglottis.
A stalk like process of epiglottis (petiole) attaches the
epiglottis to the thyroid angle.
Ant surface of the epiglottis is seperated from thyrohyoid
membrane and upper part of the thyroid cartilage y a potential
space called as the pre-epiglottic space which may be
invaded in ca of supraglottic larynx or the base of the tongue.
14.
15. ARYTENOID CARTILAGE:
these are paired Triangular pieces, hyaline cartilage located
at the posterior, superior border of the cricoid cartilage at the
back of the larynx.
It is pyramidal in form and has three surface, a base and a
apex.
Base articulates with the cricoid cartilage.
Muscular process gives attachment to the intrinsic muscles
and the vocal process gives attachment to the vocal cord and
apex supports corniculate cartilage.
16. CORNICULATE CARTILAGES:
Two small conical nodules
horn shaped , fibroelastic cartilage.
Each articulates with the apex of arytenoid cartilage.
17. CUNEIFORM CARTILAGES:
These are rod shaped each is situated in the aryepiglottic fold
in front of the corniculate cartilage and provides passive
support to the fold.
19. LARYNGEAL JOINTS:
Cricoarytenoid: it is a synovial joint formed between the
base of arytenoid and a facet.
2 movements occurs
Rotatory: AC moves in vertical axis thus abducting and
adducting the vocal cords.
Gliding: arytenoid glides towards the other or away from it
thus closing or opening the posterior part of glottis.
Cricothyroid joint: synovial joint, formed by the inferior
cornu of thyroid cartilage with a facet on cricoid cartilage.
20. LARYNGEAL LIGAMENTS:
INTRINSIC:
Cricovocal membrane: it is a triangular fibroelastic
membrane.
Its upper border forms the vocal ligament
Its lower border forms the conus elasticus where subglottic
foreign bodies get impacted.
Quadrangular membrane: lies deep to the mucosa of
aryepiglottic folds.
Stretches between the epiglottic and arytenoid cartilages.
Lower border forms the vestibular ligament which lies in the
false vocal cord.
21.
22. EXTRINSIC LIGAMENTS:
Thyrohyoid membrane: connects thyroid cartilage to
hyoid bone. Pierced by superior laryngeal vessels and
laryngeal nerve.
Cricothyroid membrane: connects thyroid cartilage to
the cricoid cartilage
Cricotracheal membrane: connects cricoid cartilage to
the first tracheal ring.
23. INTRINSIC LIGAMENTS:
THE CORNUS ELASTICUS-- is
composed mainly of yellow elastic tissue. It
connects the thyroid, cricoid, arytenoid cartilage to
one another .
THYROEPIGLOTTIC LIGAMENT----
is a long, slender, elastic cord which connects the
stem of the epiglottis with the angle of thyroid
cartilage.
24. MUSCLES OF LARYNX:
Extrinsic muscles (attaches larynx to the surrounding
structures)
•divided into the elevators and depressors of larynx:
Elevators: primary elevators act directly as they are attached
to the thyroid cartilage includes stylopharyngeus,
salpingopharyngeus, palatopharyngeus and thyrohyoid.
25. Secondary elevators: they act indirectly as they are
attached to the hyoid bone and includes mylohyoid, digastric,
stylohyoid and geniohyoid.
Depressors: they include sternohyoid, sternothyroid and
omohyoid.
26. EXTRINSIC MUSCLES:
The Geniohyoid Muscle
They lie superior to the mylohyoid muscle to body
of the hyoid bone
The Stylohyoid Muscle
Insertion: the body of the hyoid bone
27. The thyrohyoid
muscle - It arises from the oblique line on the
lamina of the thyroid cartilage, and to the
greater cornu of the hyoid bone.
28. INTRINSIC MUSCLES OF LARYNX:
Acts on the vc and laryngeal inlet.
Those acting on the vc:
Abductors: posterior cricoarytenoid
Adductors: lateral cricoarytenoid, interarytenoid and
thyroarytenoid
Tensors: cricothyroid vocalis
Those acting on the laryngeal inlet:
Openers of LI: thyroepiglottic
Closers: interarytenoid and aryepiglottic.
29.
30. CAVITY OF THE LARYNX: it starts at the laryngeal inlet
where it communicates with the pharynx and ends at the lower
border of cricoid cartilage where it continues with the lumen of
the trachea.
2 pairs of folds vestibular and vocal divides the cavity into the
3 parts:
• Divided into 3 parts:
– Vestibule
– Ventricle (sinus of larynx)
– Subglottic space (infraglottic larynx) extends from the vc to
the lower border of cricoid cartilage.
31. False vocal cords (vestibular folds): 2 in no these
are fold of mucous membrane contains vestibular ligament,
fibers of thyroarytenoid muscle and mucus glands.
True vocal cords: (vocal folds): pearly white sharp
bands extending from the middle of the thyroid angle to the
vocal process of arytenoid. Each vc consists of vocal
ligament.
Glottis: (rima glottidis): elongated space between vocal
cords anteriorly and vocal processes post
24mm in males 16mm in females.
32.
33. Reinke’s space:
Under the epithelium of vocal cord is a potential space with
scanty subepithelial connective tissues bounded above and
below by arcuate lines, infront by ant comissure and behind
by vocal process of arytenoid. oedema of this space causes
fusiform swelling of the membranous cords.
37. NERVE SUPPLY:
Motor supply: recurrent laryngeal nerve
Sensory nerve supply up to the vocal fold is internal
laryngeal nerve and below the vocal is recurrent
laryngeal nerve.