Download as PDF, PPTX
![O Warda
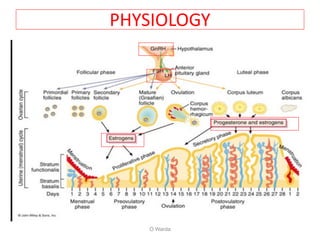
Negative Pregnancy.test
TSH ,PRL,
P4 challenge test
+VE withdrawal
bleeding
without withdrawal
bleeding
hypoestrogenic compromised
outflow tract
+ve.est/progest
challenge test -ve.est/progest
challenge test
FSH>30-40
Normal FSH
HSG OR hysteroscopy
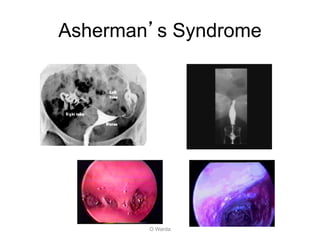
Asherman’s
FSH norm.
repeat
Repeat [+] serum
estrogen level
POFhypothalamic-
pituitary failure
Anovulation](https://image.slidesharecdn.com/amenorrhea-201216044532/85/Amenorrhea-warda-33-320.jpg)

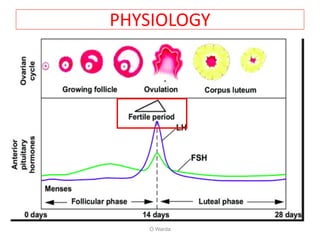
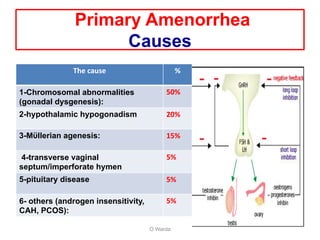
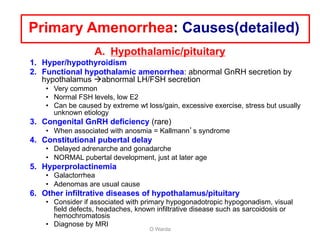
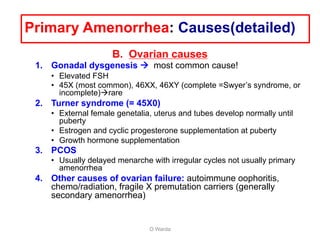
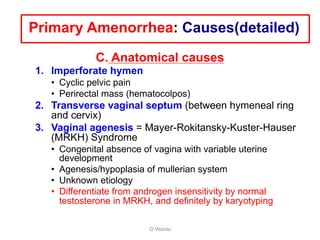
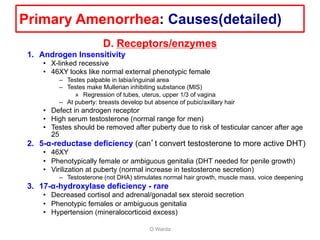
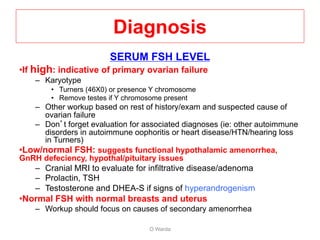
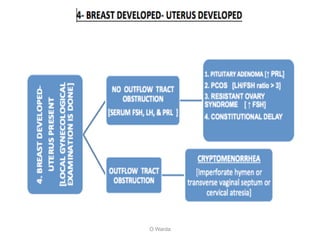
Primary amenorrhea is defined as the absence of menstruation by age 14 with no secondary sex characteristics or by age 16 with or without secondary sex characteristics. Secondary amenorrhea is defined as the absence of menstruation for 6 months or more after menstruating previously. The document provides detailed information on the causes, diagnosis, and treatment of primary and secondary amenorrhea. For primary amenorrhea, the most common causes are chromosomal abnormalities, hypothalamic hypogonadism, and Mullerian agenesis. The diagnosis involves assessing secondary sex characteristics, family history, laboratory tests of FSH, prolactin and thyroid levels, and imaging tests. Treatment focuses on treating the underlying cause and replacing any


































![Primary Amenorrhoea in Gynecologyamenorrhea[1].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/amenorrhea1-250624124653-9447ebcf-thumbnail.jpg?width=640&height=640&fit=bounds)




















































