Downloaded 122 times
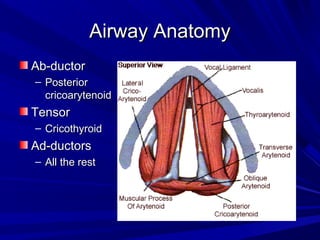

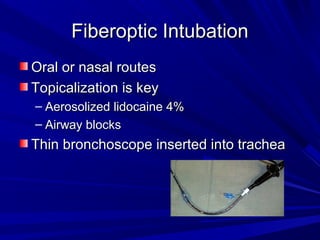
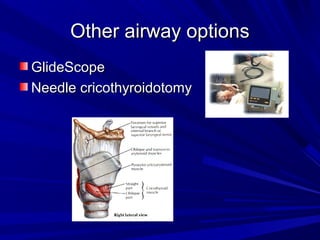

The document reviews airway anatomy, evaluation techniques for predicting a difficult airway, methods for mask ventilation and endotracheal intubation, challenges that may be encountered during intubation and how to address them, as well as other airway management techniques like using a LMA or performing a fiberoptic intubation when direct laryngoscopy is not possible. Proper preparation, skills, and following an algorithm are emphasized for safely managing routine and difficult airways.























































































