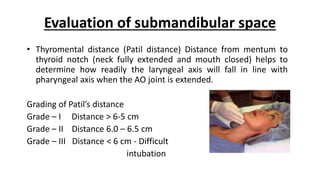
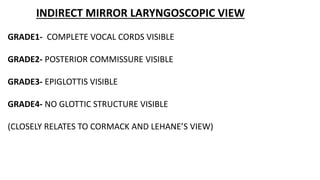
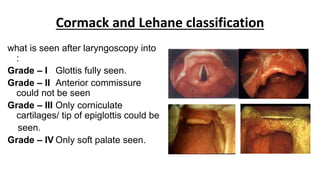
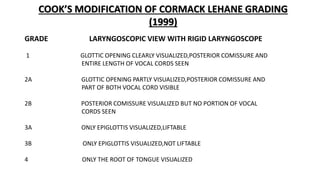
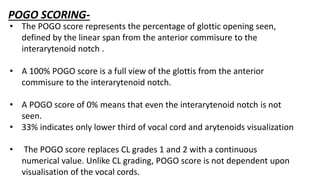
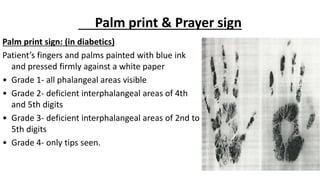
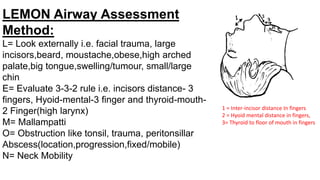
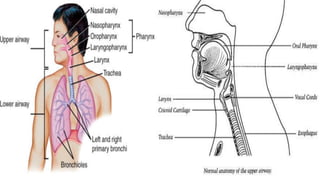
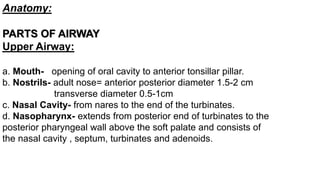
Upper airway anatomy includes the mouth, nasal cavity, nasopharynx, oropharynx, larynx, and lower airway including the trachea and bronchi. Factors predisposing to a difficult airway include congenital deformities, infections, tumors, arthritis, and injuries. A thorough airway assessment involves history, physical exam including focused tests like Mallampatti score, thyromental distance, jaw mobility, and neck range of motion to identify potential difficulties and plan management.

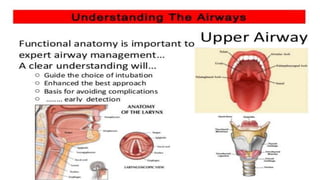
![Oropharynx- extends from soft palate above to epiglottis below and anteriorly from
anterior tonsillar pillar to posterior pharyngeal wall , it includes tonsil,uvula and the
epiglottis.
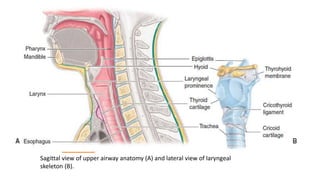
Pharynx-The pharynx is a U-shaped fibromuscular tube that extends from the base of
the skull to the cricoid cartilage. It is bounded anteriorly and superiorly by the nasal
cavity, followed more inferiorly by the mouth, and then the larynx. These borders divide
the pharynx into the nasopharynx, oropharynx, and laryngopharynx, respectively.
Larynx- extends form laryngeal inlet i.e C3-C4 to lower border of cricoid cartilage (C5-
C6)-[ Importance :Phonation and Swallowing ]
Contents :
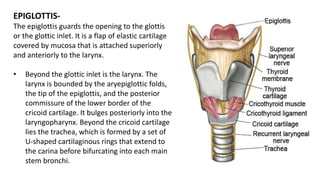
Unpaired Cartilage = Thyroid , Cricoid and Epiglottis ,
Paired =Arytenoid , Corniculate and Cuneiform (most vulnerable area for obstruction
and trauma during laryngoscopy)](https://image.slidesharecdn.com/airwayassesment-180820095455/85/Airway-assesment-IN-ANESTHESIA-6-320.jpg)
![• History
patient notes /chart/ medic alert
• Surgery /burns
• Concurrent disease
• Reflex disease/recent meals
General examination
• Dentition[pominent upper incisors,receding chin]
• Distortion[ edema,blood,vomit,tumor,inection]
• Disproportion[short chin-to-larynx distance, bull neck,large tongue, small mouth]
• Dysmobility[TMJ and cervical spine]
• Massively obese or pregnant
• beards/tubes
Specific tests/indices
Investigations
• Nasoendoscopy/FLUROSCOPY
• X-ray, CT/MRI/USG
• Flow volume loop](https://image.slidesharecdn.com/airwayassesment-180820095455/85/Airway-assesment-IN-ANESTHESIA-23-320.jpg)