Download as PDF, PPTX
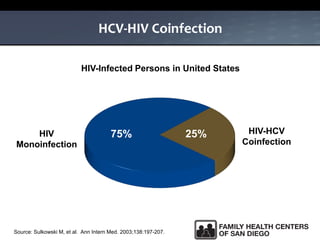
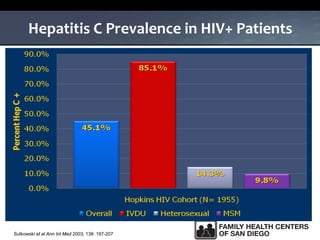
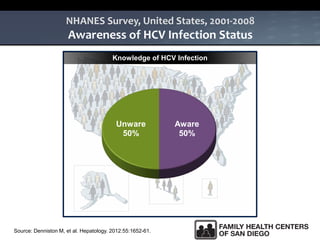
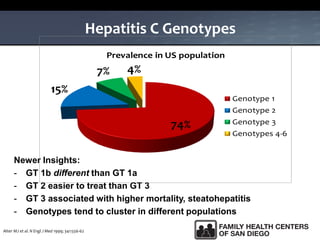
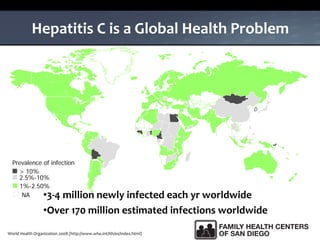
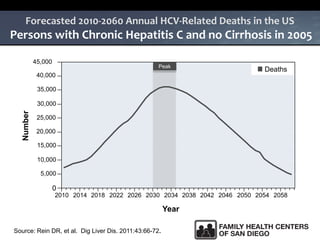
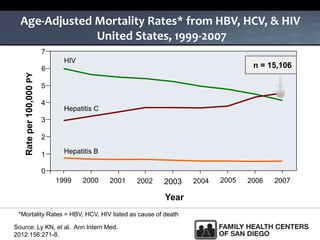



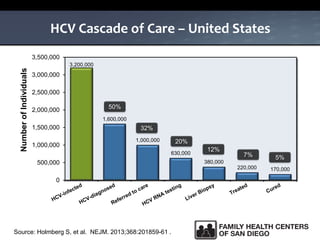




The UC San Diego Antiviral Research Center hosts weekly presentations to share the latest research and clinical practices related to various infectious diseases, including HIV and Hepatitis C (HCV). The document highlights key findings on HCV epidemiology, transmission risks, and screening recommendations, especially focused on community health settings. It also discusses the significant burden of HCV-related mortality and the urgent need for effective screening and treatment strategies in the San Diego region.


























































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)















