Download to read offline


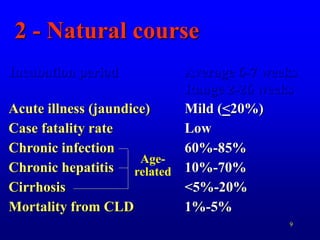
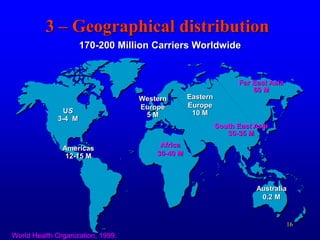
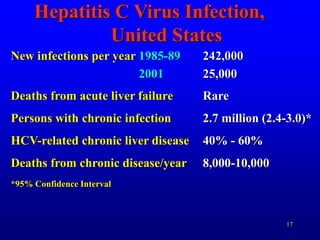
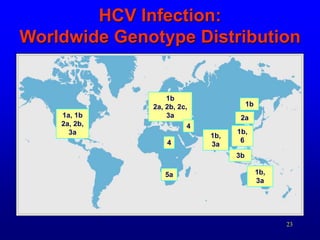
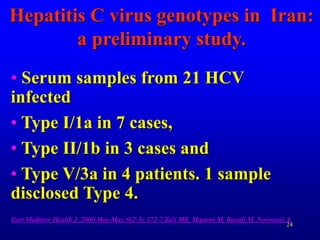
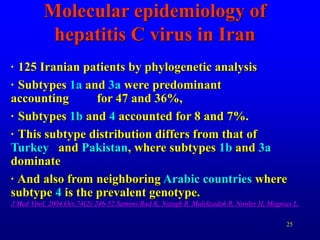

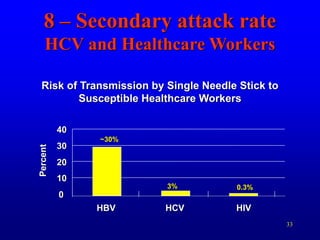
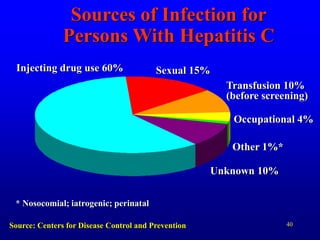

This document summarizes key information about hepatitis C virus (HCV) epidemiology. It discusses: 1) HCV is a bloodborne virus that commonly causes chronic liver disease. It has six major genotypes that predict treatment outcomes. 2) HCV has a worldwide prevalence of 170-200 million carriers. The highest prevalence is in Egypt, while the US has an estimated 2.7 million carriers. In Iran, genotypes 1a and 3a are most common. 3) HCV transmission occurs primarily through injection drug use and, historically, blood transfusions. Occupational and perinatal transmission are less common. Prevention focuses on screening blood and injection safety.





















































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)













