







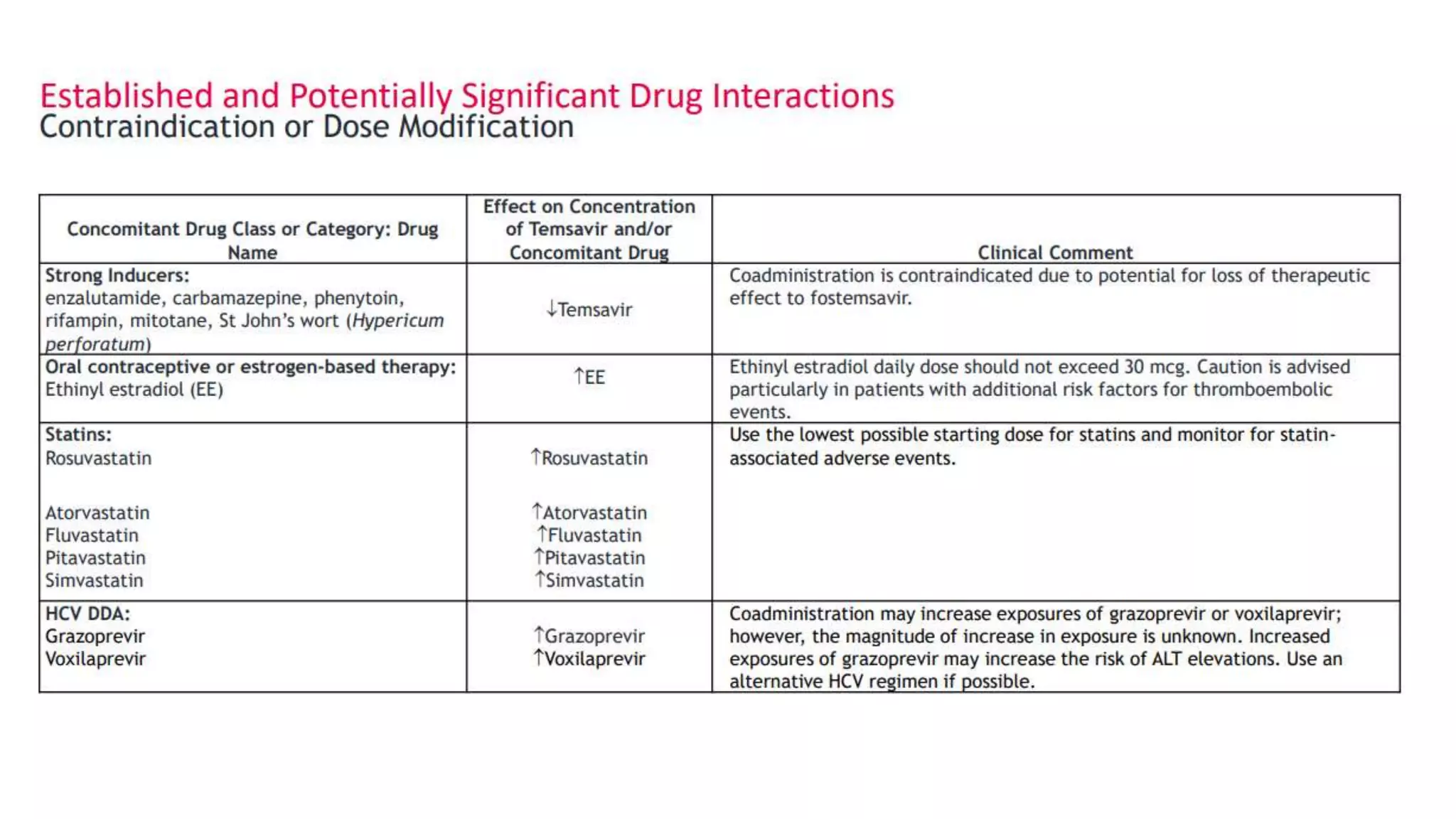






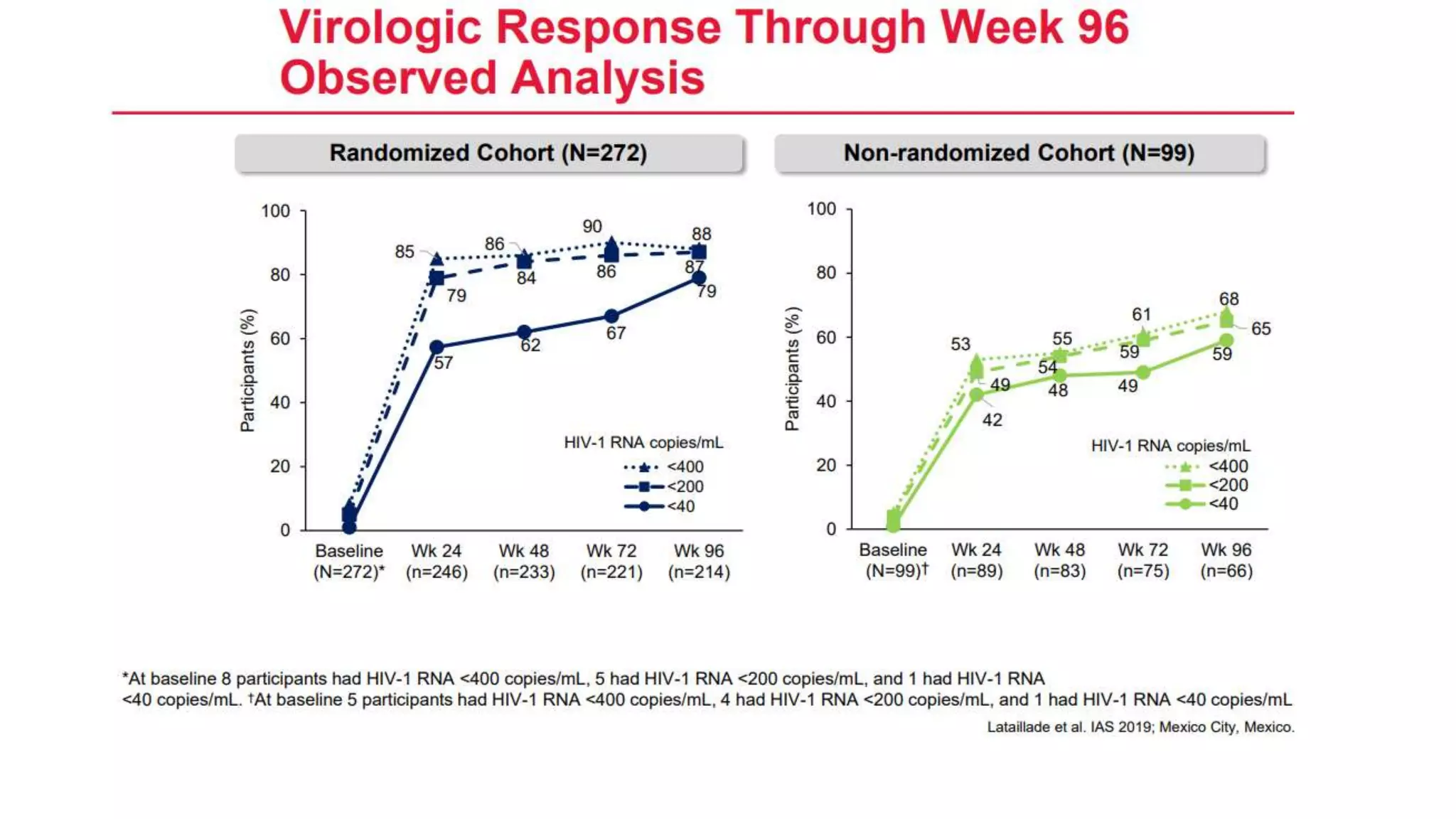



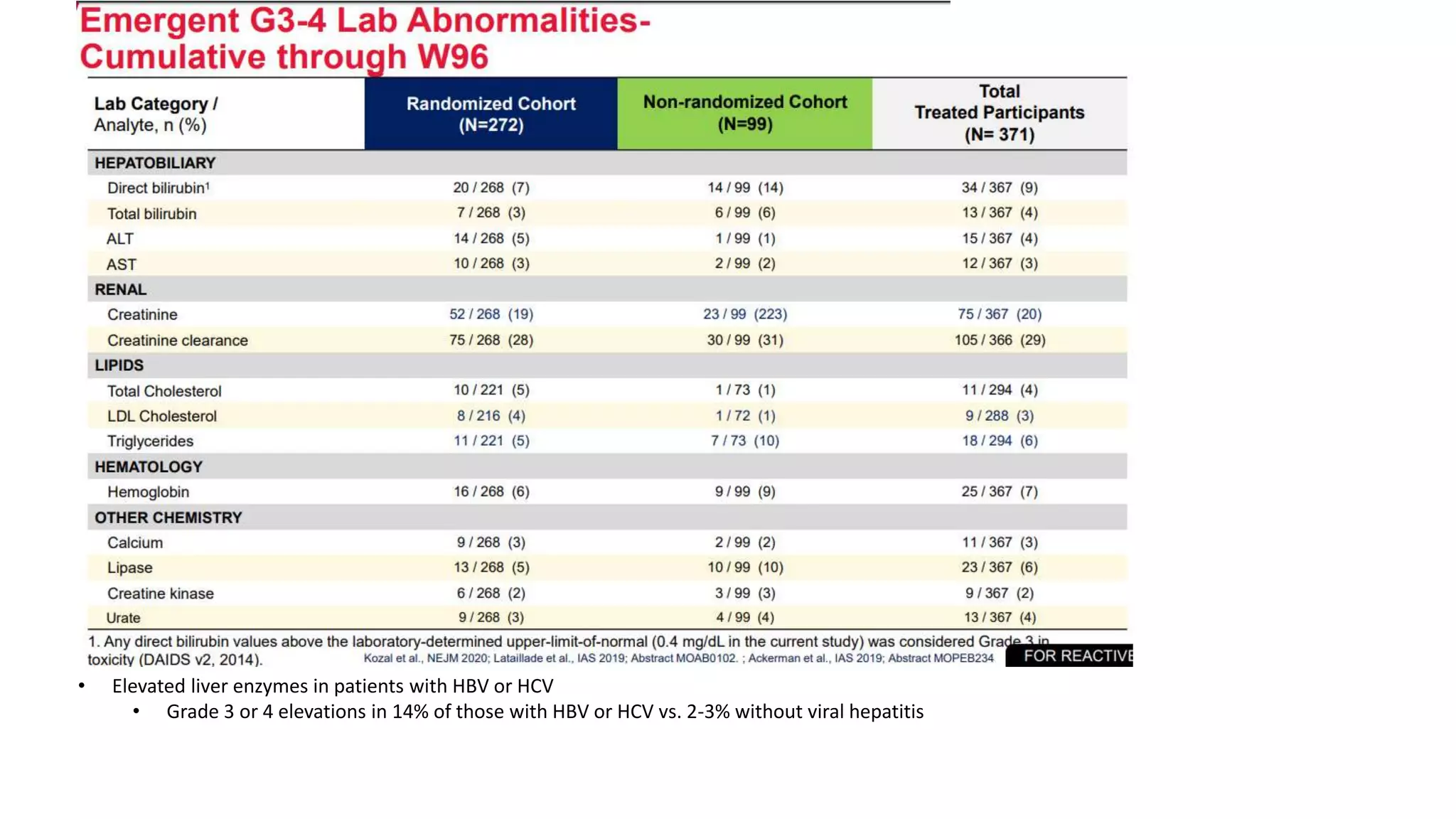
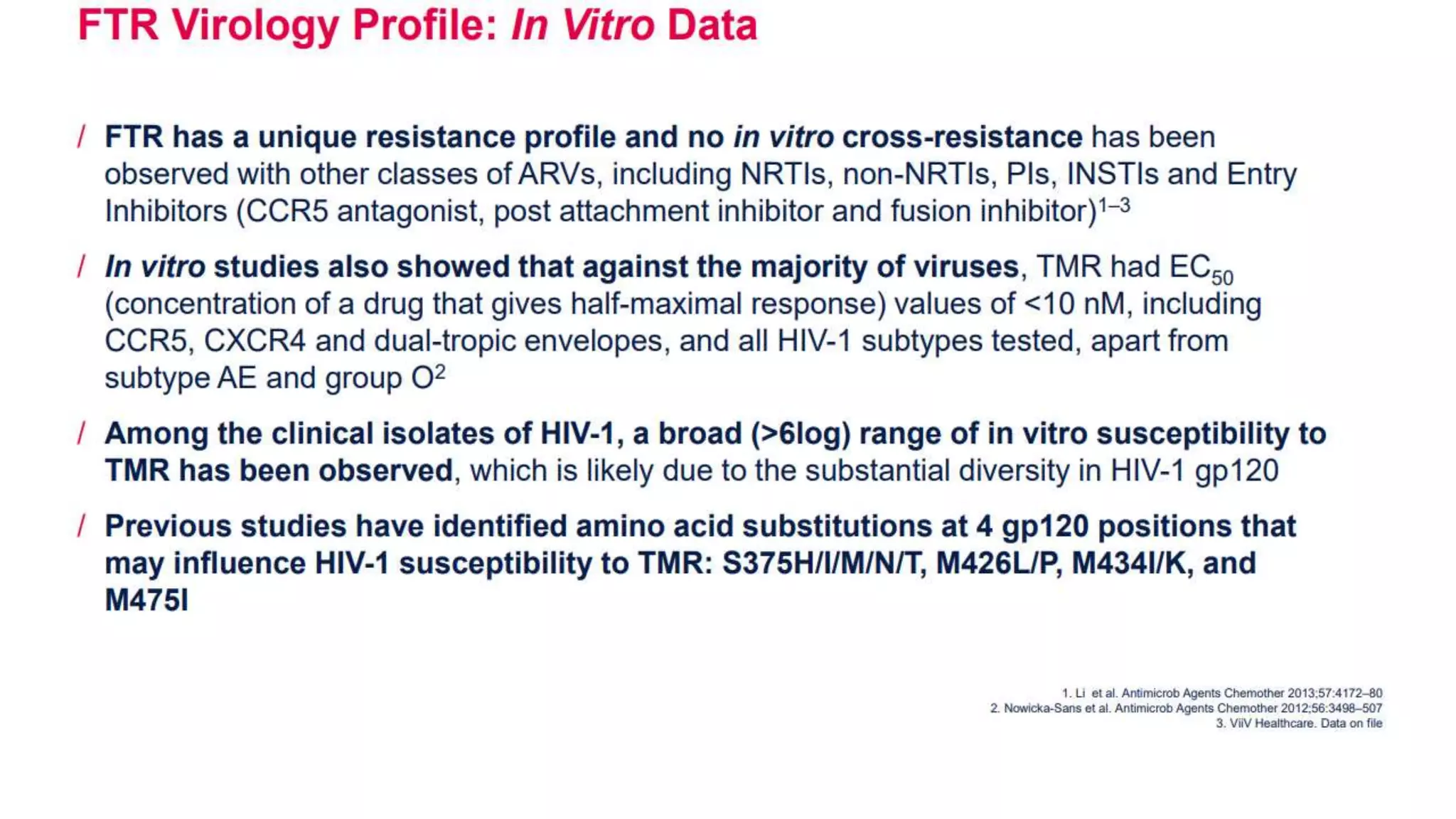

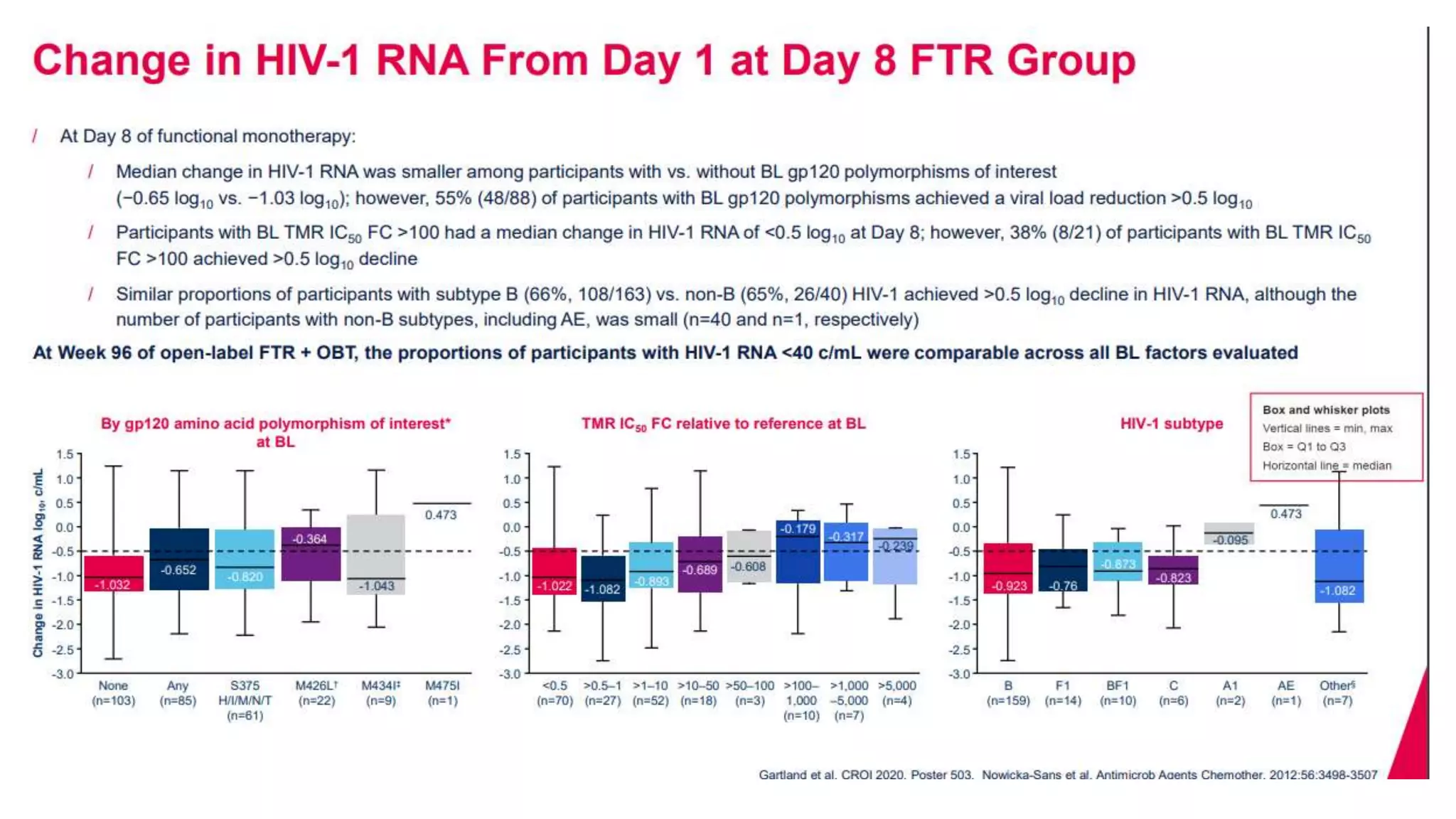







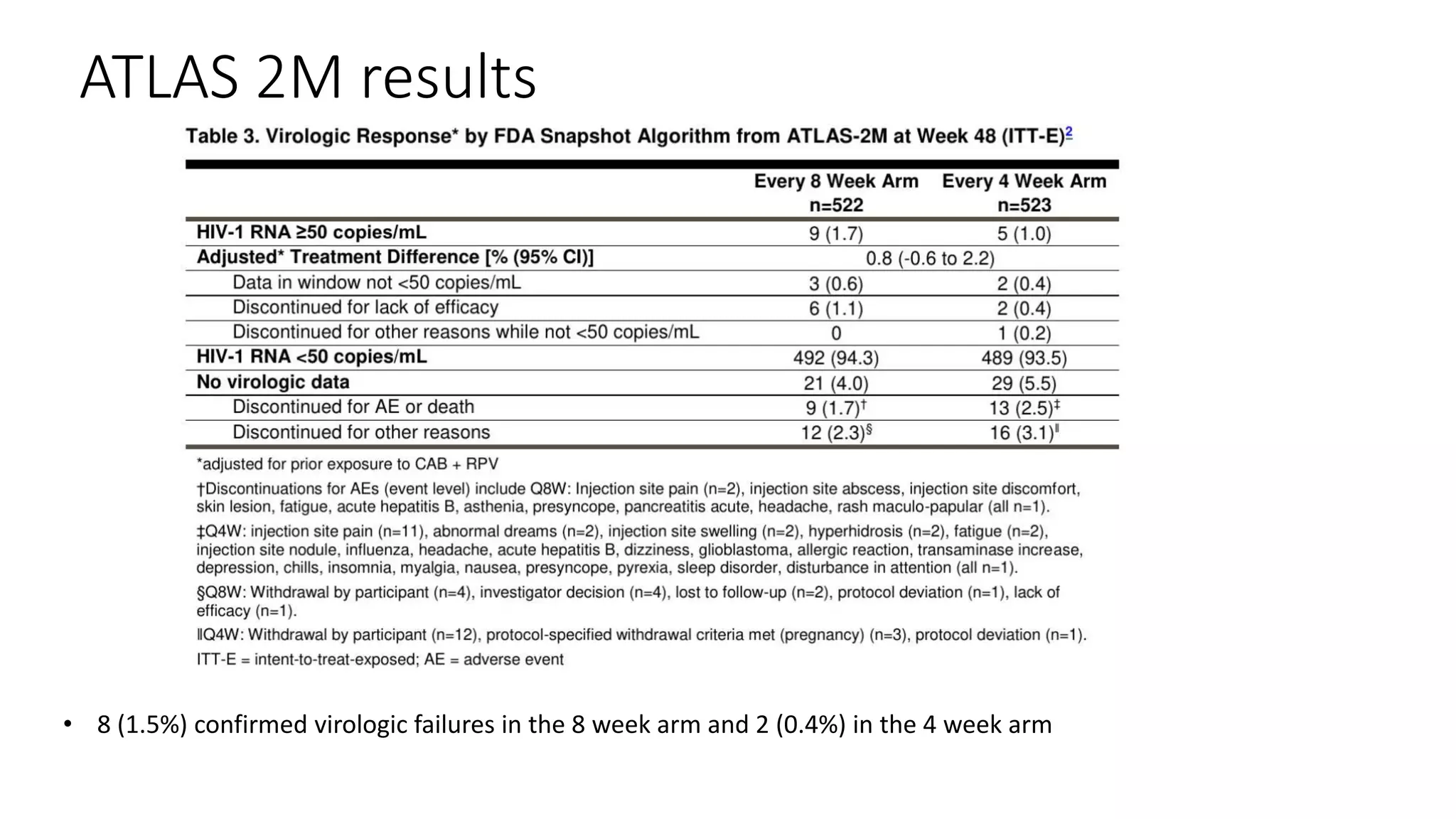





















This document summarizes a presentation on new and investigational antiretrovirals given at the UC San Diego HIV & Global Health Rounds. The presentation reviewed fostemsavir, cabotegravir/rilpivirine, leronlimab, islatravir, and lenacapavir. For each drug, the presenter discussed indications, dosing, efficacy and safety data from clinical trials, resistance profiles, and potential advantages and limitations. The goal of the HIV & Global Health Rounds is to provide clinicians and researchers with the most up-to-date information on HIV, hepatitis, tuberculosis, and other infectious diseases.









































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)













