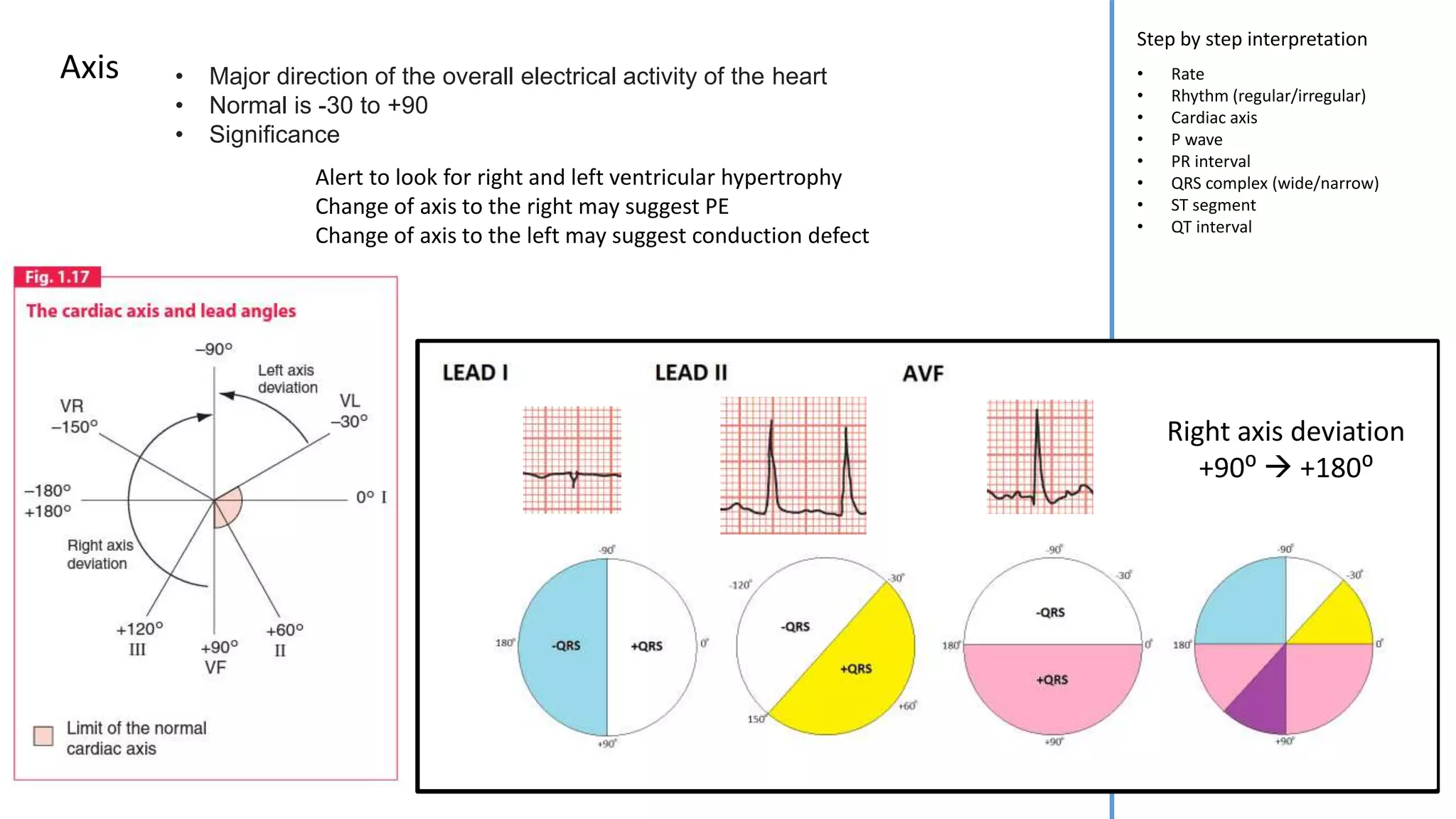
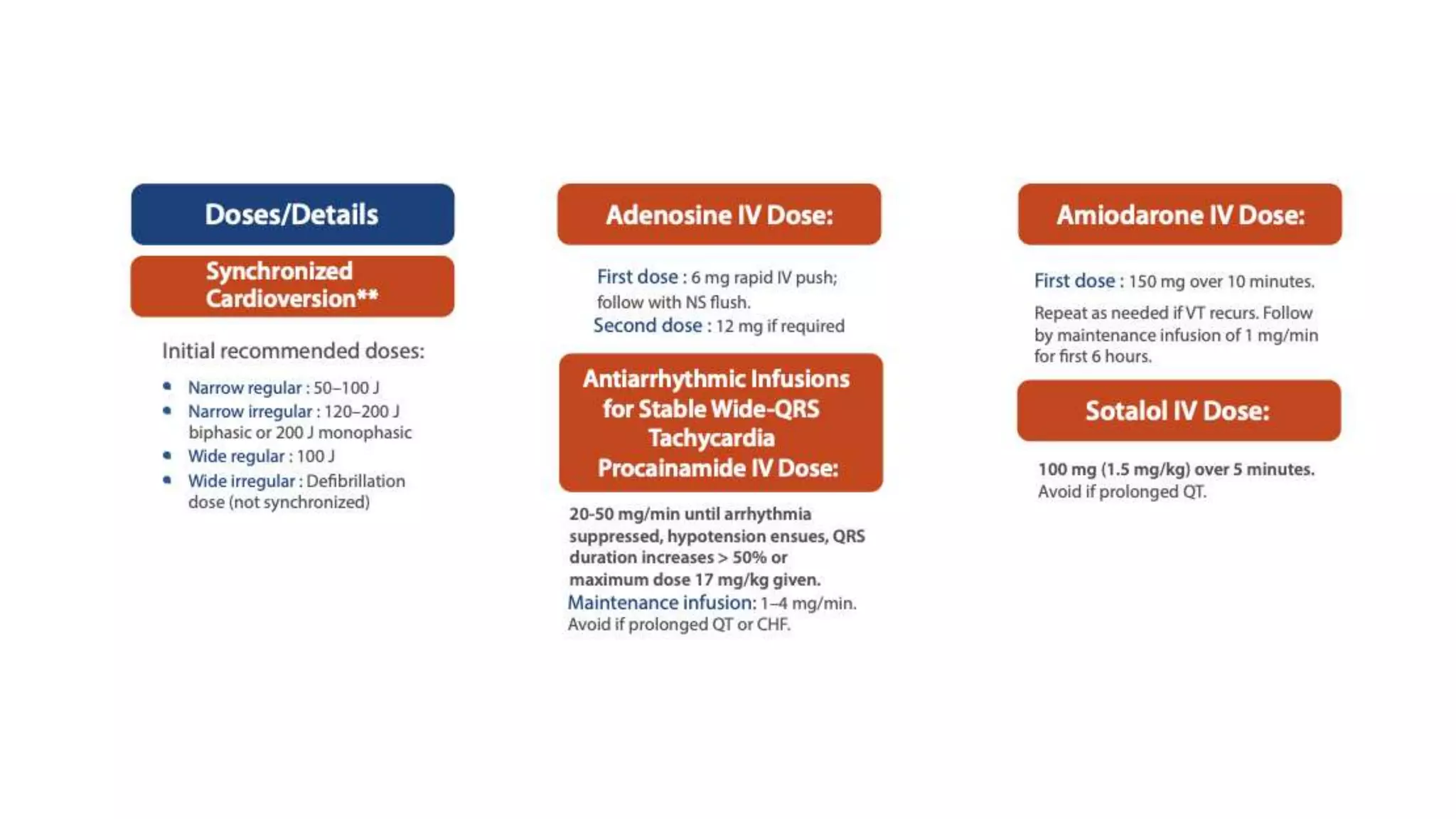
This document provides information on cardiac rhythm recognition and management according to advanced cardiac life support protocols. It defines key ECG parameters such as rate, rhythm, P waves, QRS complexes and intervals. It outlines a step-by-step approach to ECG interpretation and describes the treatment of various cardiac arrhythmias and arrests including defibrillation, cardioversion, transcutaneous pacing and management of conditions like supraventricular tachycardia, atrial fibrillation, ventricular tachycardia and bradyarrhythmias. Reversible causes of cardiac arrest are also listed.