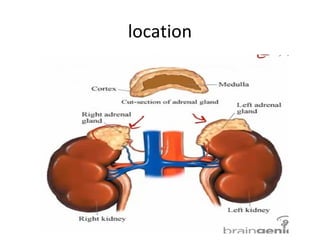
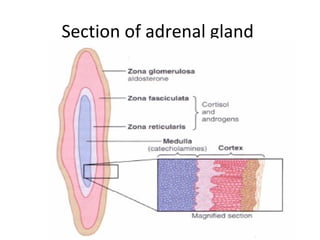
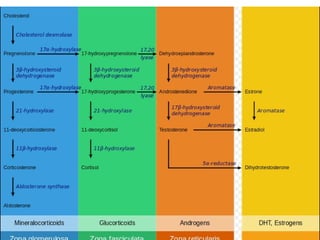
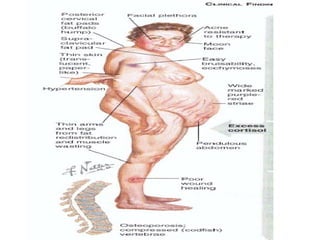
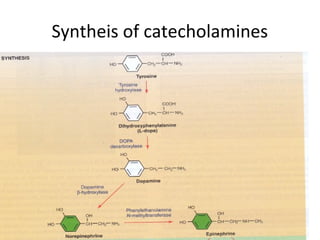
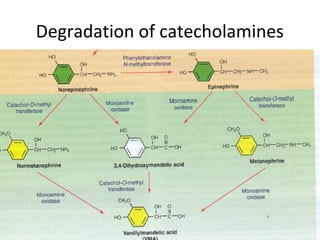
The adrenal glands are located above the kidneys and are composed of the adrenal cortex and medulla. The cortex secretes mineralocorticoids like aldosterone and glucocorticoids like cortisol. It also secretes small amounts of adrenal androgens. The medulla secretes catecholamines such as epinephrine and norepinephrine in response to sympathetic stimulation. Diseases of the adrenal glands can result in either hypo- or hypersecretion of hormones with various clinical effects.