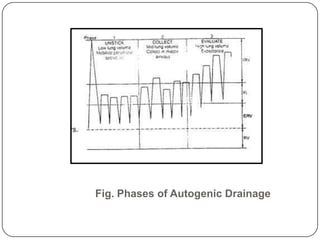
Autogenic drainage (AD) is a controlled breathing technique, developed in Belgium during the late 1960s, aimed at clearing chest secretions without excessive coughing. The process involves three phases: 'unsticking' secretions through low breathing, 'collecting' them in mid-sized airways, and 'evacuating' them with high-volume breaths. The technique is designed for patients with retained secretions, particularly beneficial for children, while precautions must be taken for certain medical conditions.

























































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)










![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)






