Downloaded 2,570 times
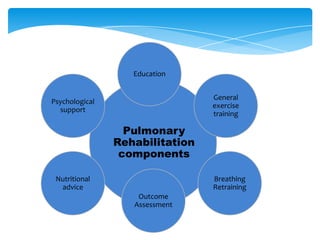
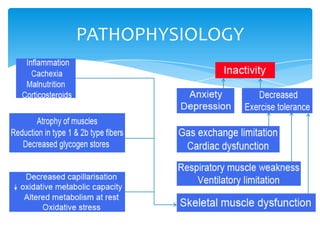


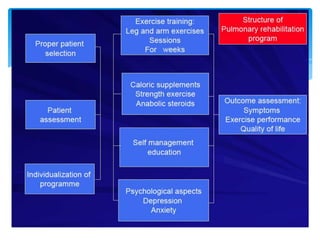




This document provides an overview of pulmonary rehabilitation. It begins by defining pulmonary rehabilitation and describing its goals. It then discusses the various components of pulmonary rehabilitation including education, exercise training, psychosocial support, nutritional counseling, and outcome assessment. The document outlines the pathophysiology targeted by pulmonary rehabilitation and reviews evidence on the benefits of the various components. It provides guidance from professional societies on elements like patient selection, setting, exercise prescription and duration. Overall, the document presents pulmonary rehabilitation as a multidisciplinary program aimed at improving the physical and psychological condition of patients with chronic respiratory diseases through exercise and other therapies.























![Physiotherapy in pulmonary_surgery[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/pulmonarysurgery1-230705093621-2b78f958-thumbnail.jpg?width=640&height=640&fit=bounds)










































