Downloaded 17 times


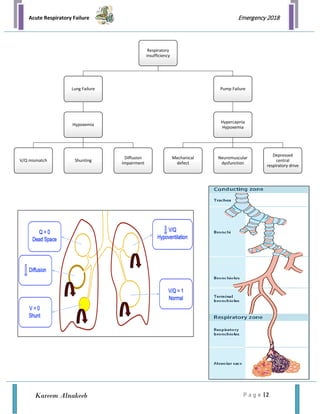






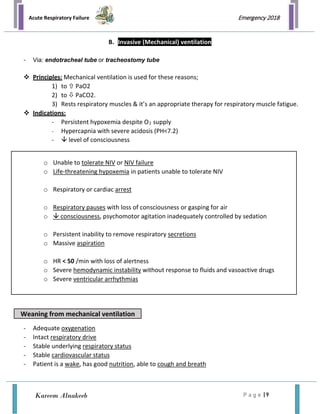
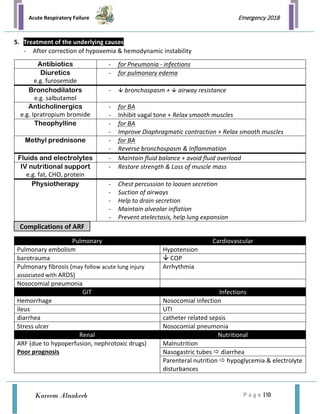

Acute respiratory failure (ARF) is a condition characterized by the failure of the respiratory system to maintain adequate gas exchange, leading to hypoxemia (low oxygen) and/or hypercapnia (high carbon dioxide). It can be classified into acute or chronic types and categorized as hypoxemic or hypercapnic. Treatment involves addressing the underlying causes, providing oxygen therapy, and potentially mechanical ventilation to ensure sufficient oxygen delivery and ventilation.