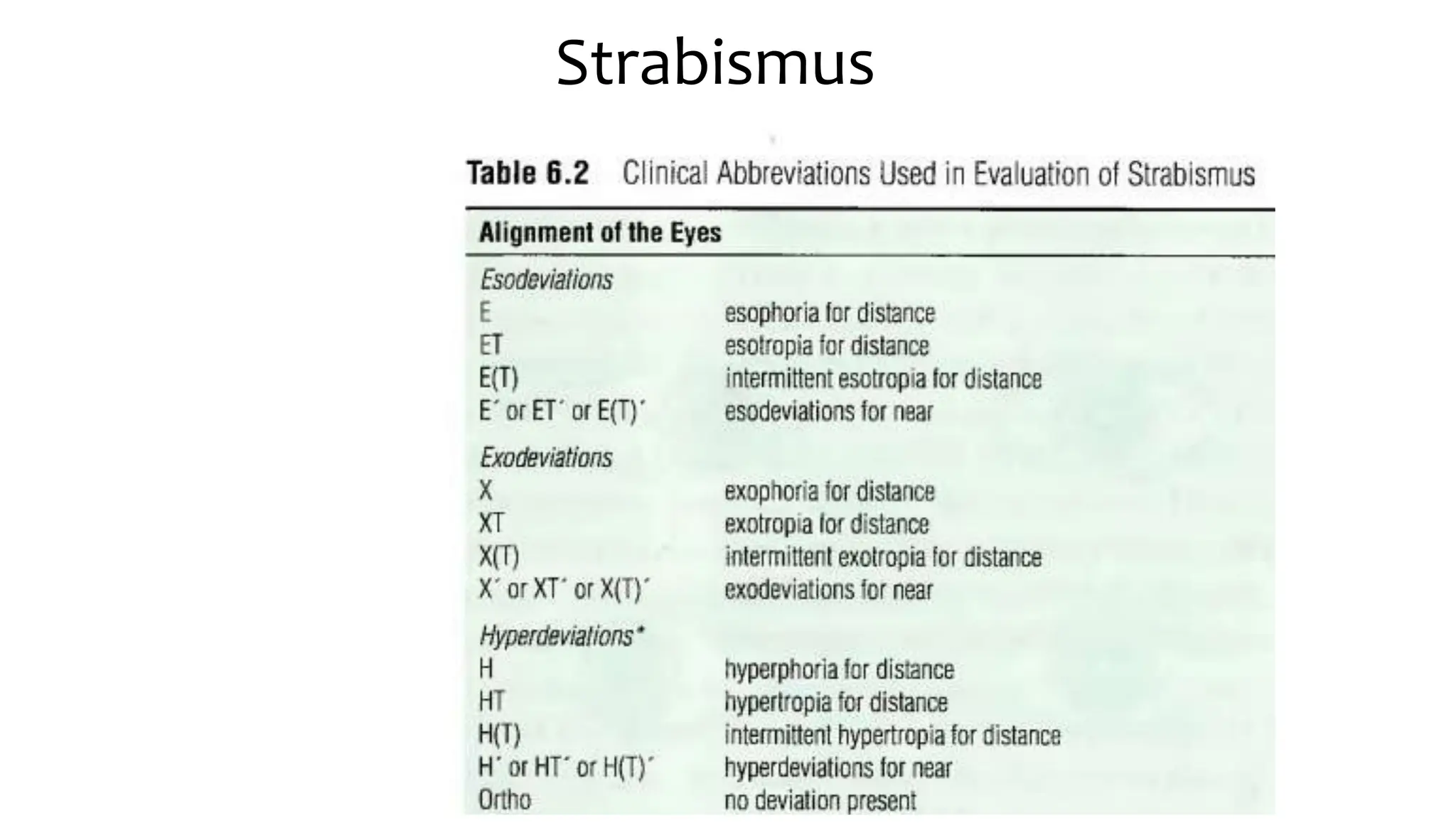
The document discusses various types of strabismus, particularly focusing on esotropia, which is the most common deviation in the pediatric population. It covers causes, risk factors, prevalence, types such as congenital and accommodative esotropia, associated conditions, and treatment options including surgical interventions and the use of botulinum toxin. Special attention is given to specific syndromes related to esotropia, such as infantile esotropia and Duane retraction syndrome, highlighting their characteristics and management strategies.