The document discusses localization of accessory pathways using electrocardiography. It describes:
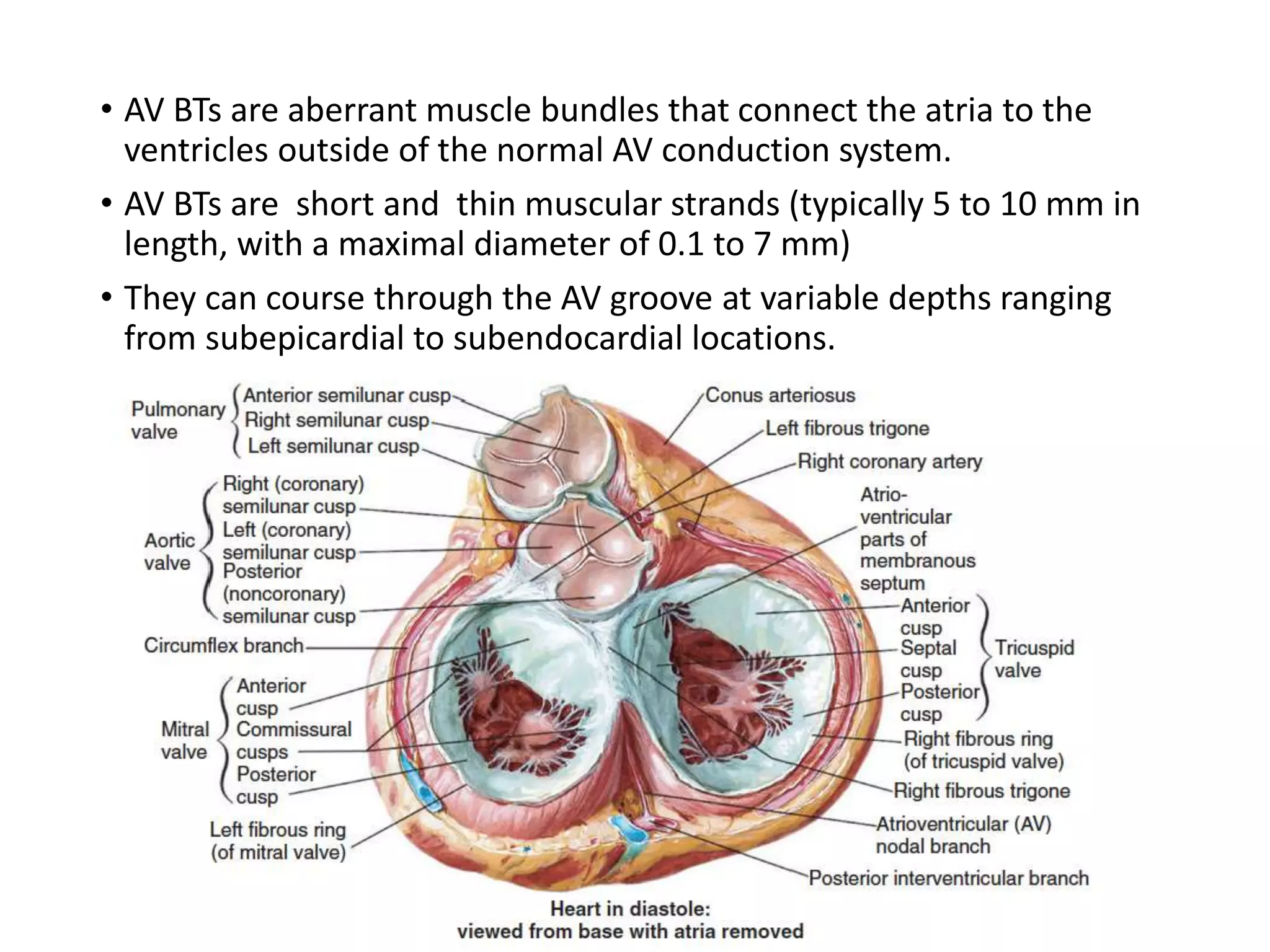
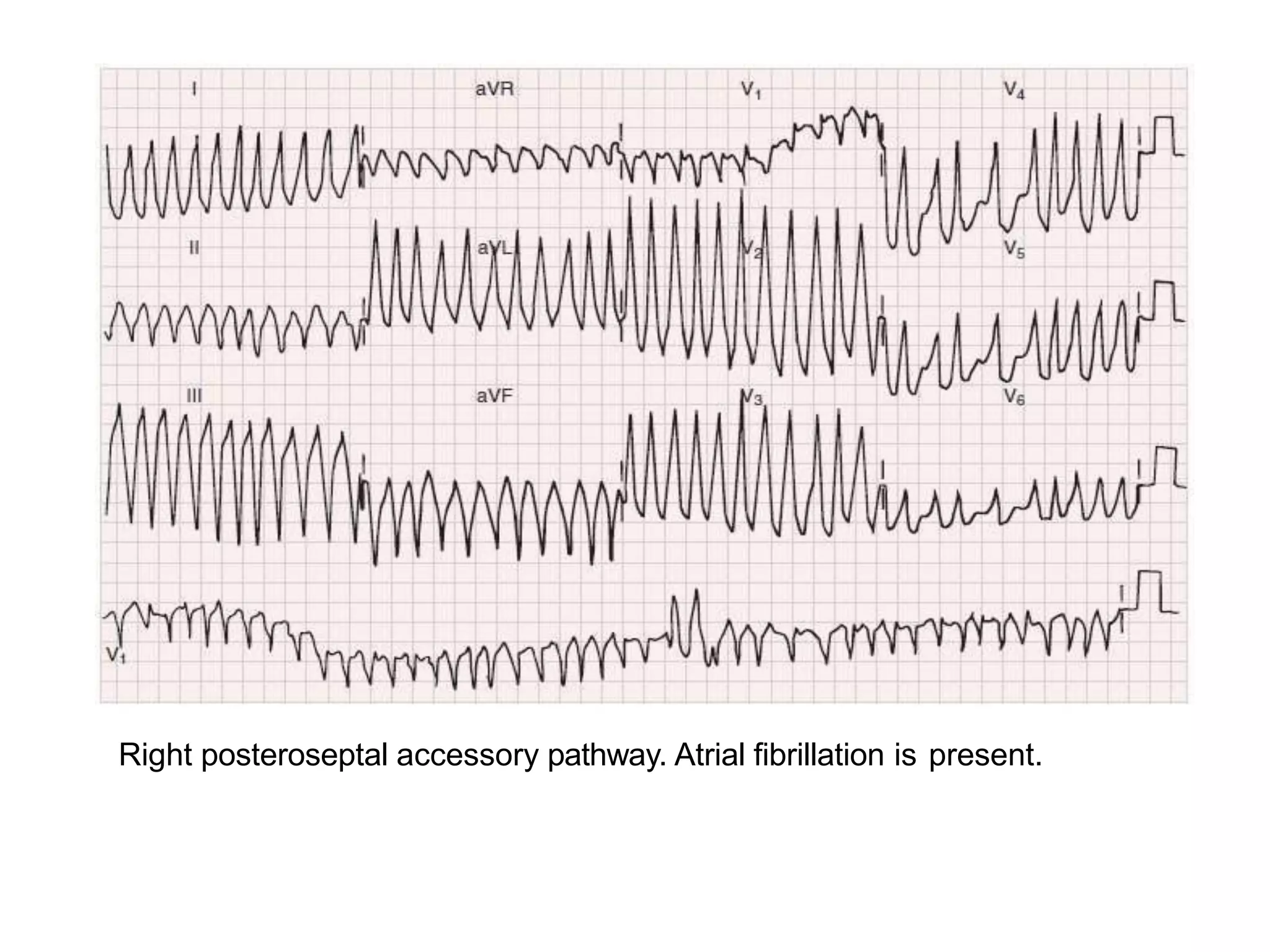
- Accessory pathways are aberrant muscle bundles connecting the atria and ventricles outside the normal conduction system.
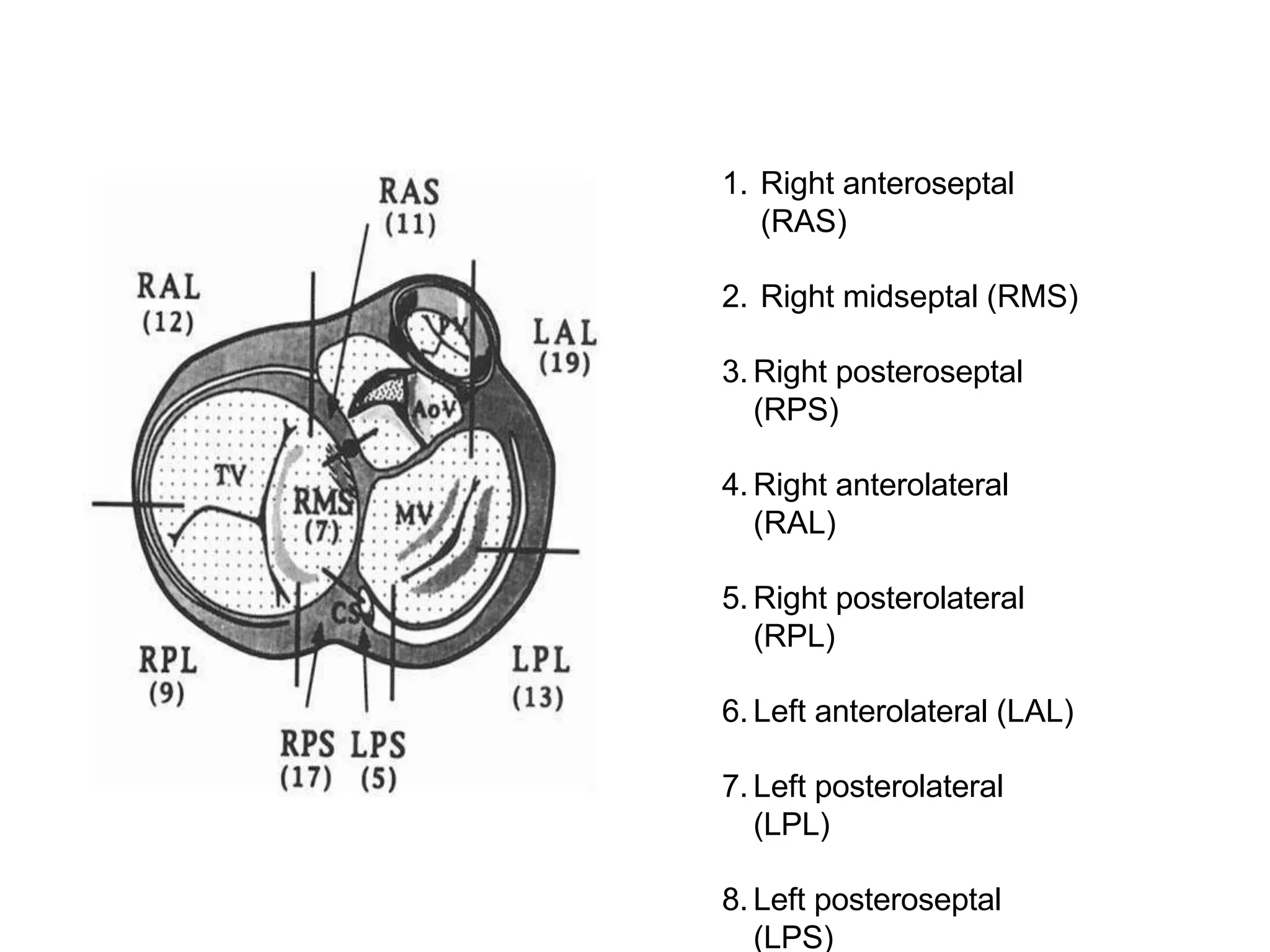
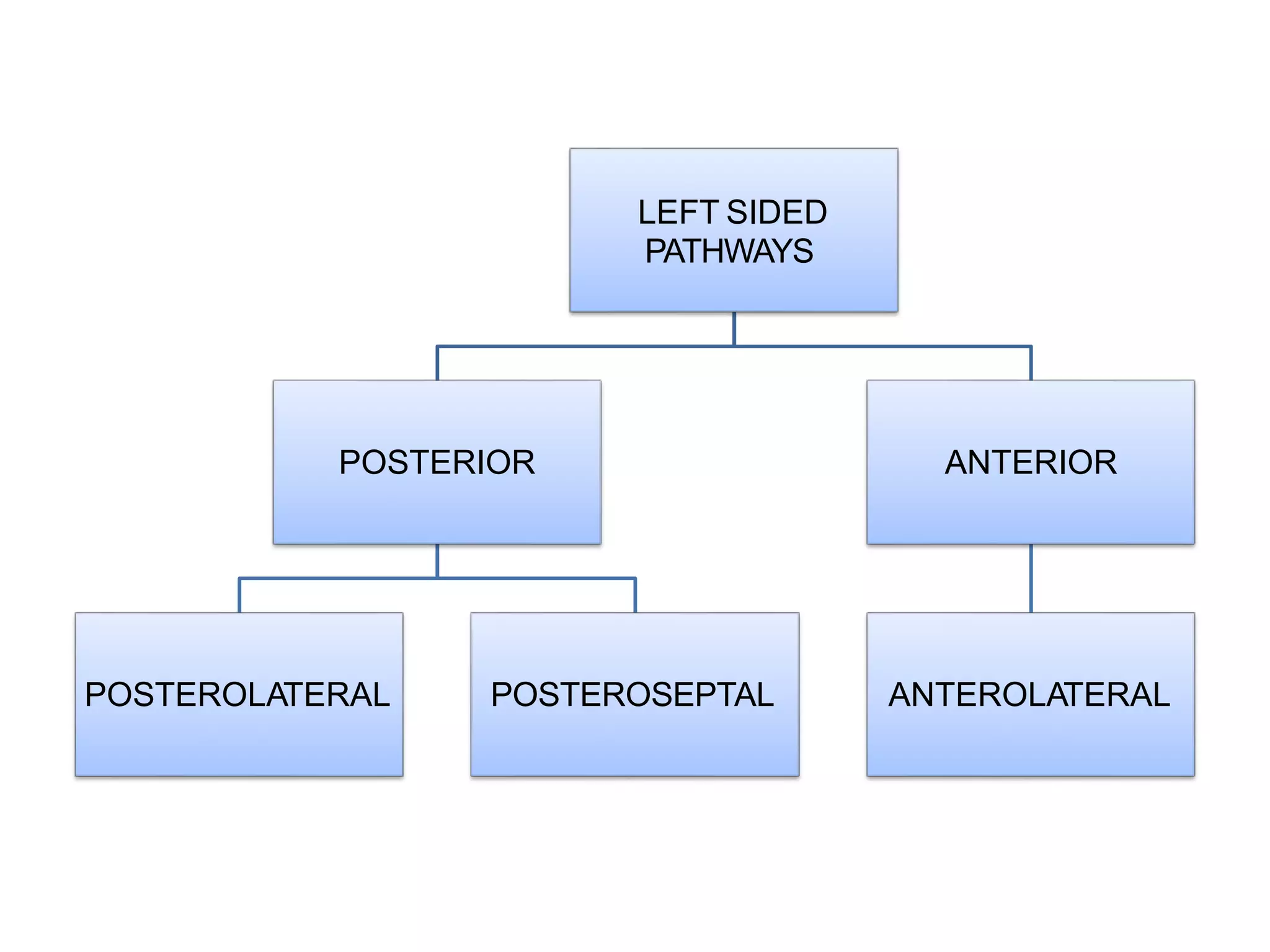
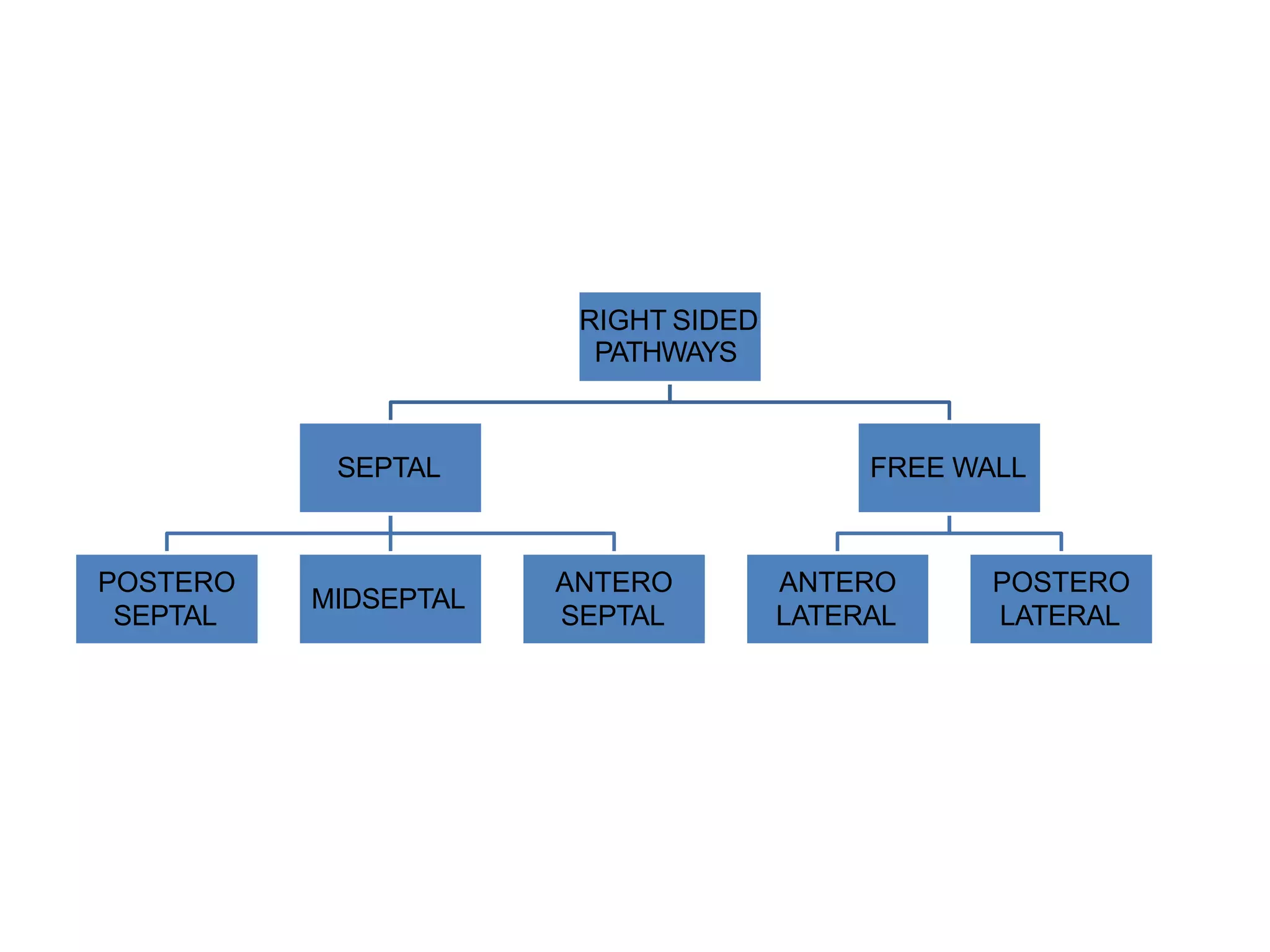
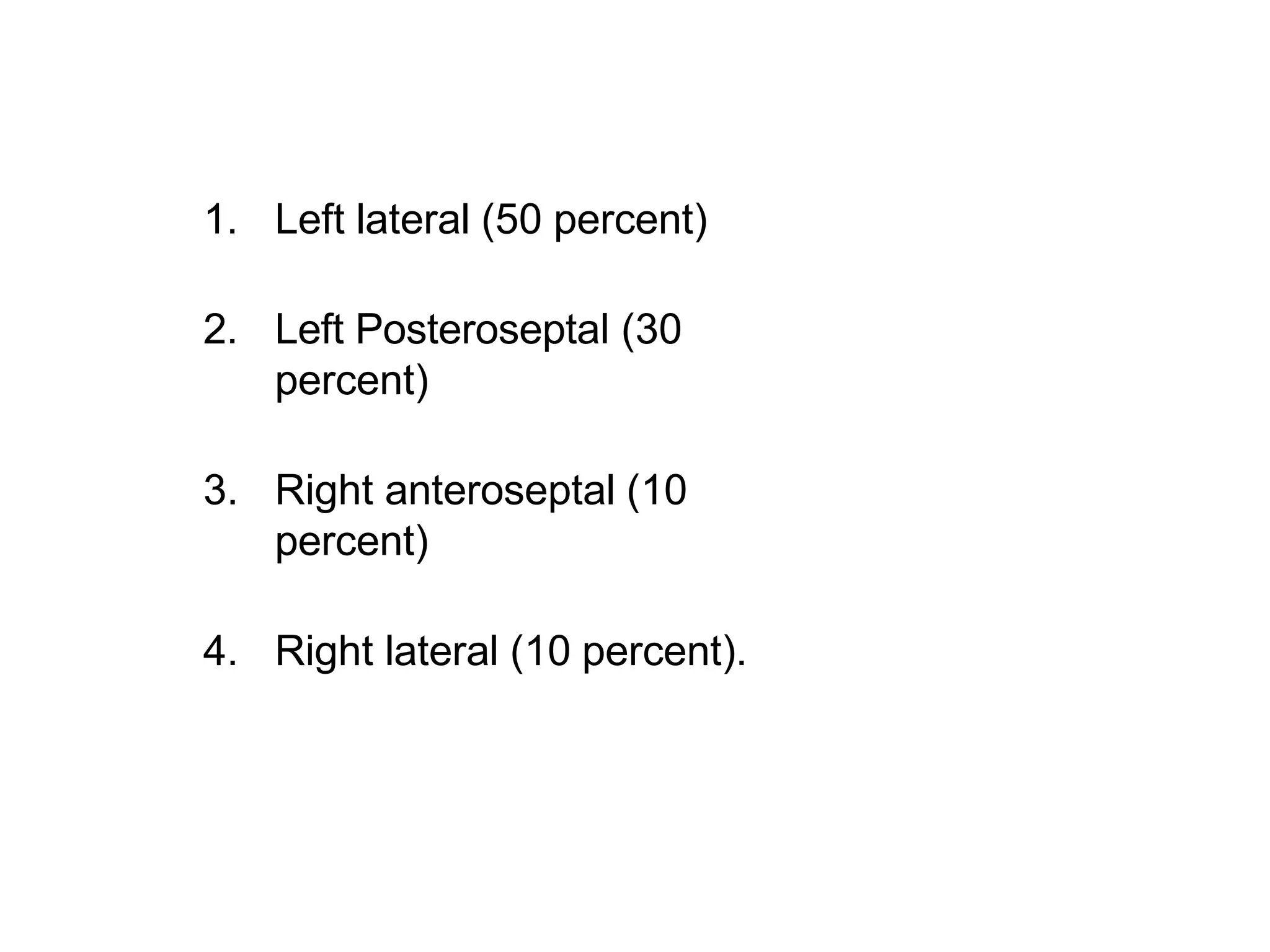
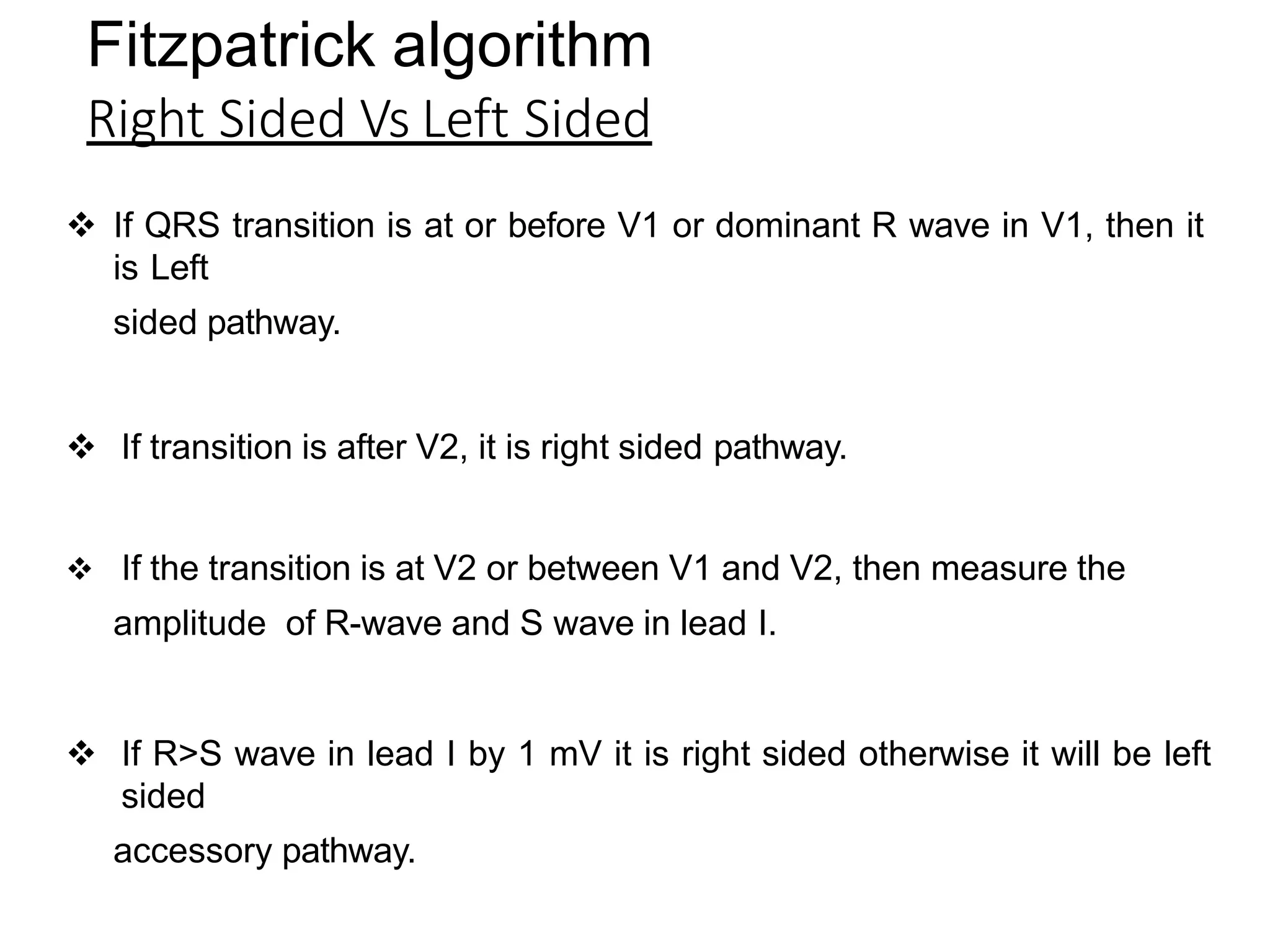
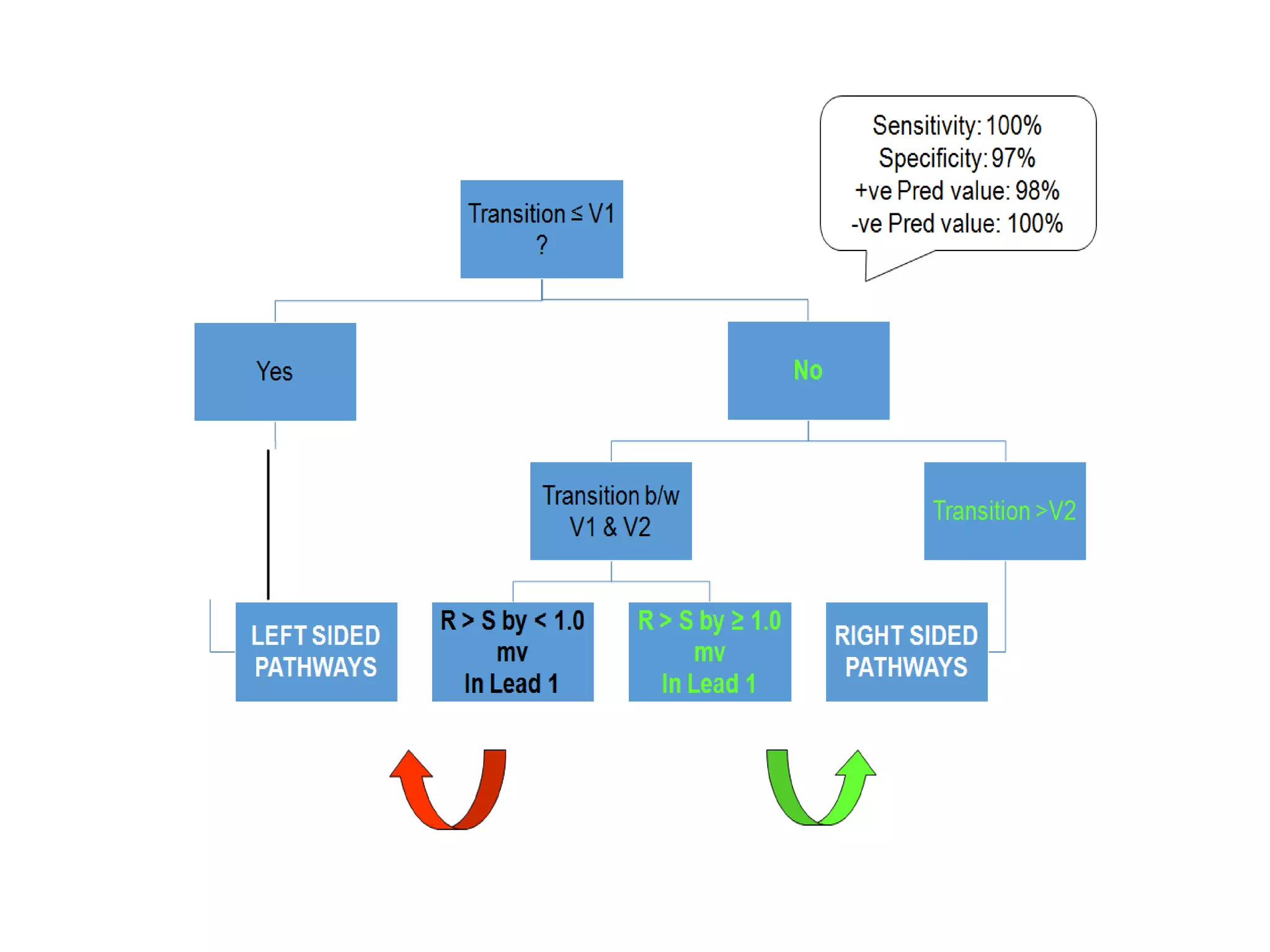
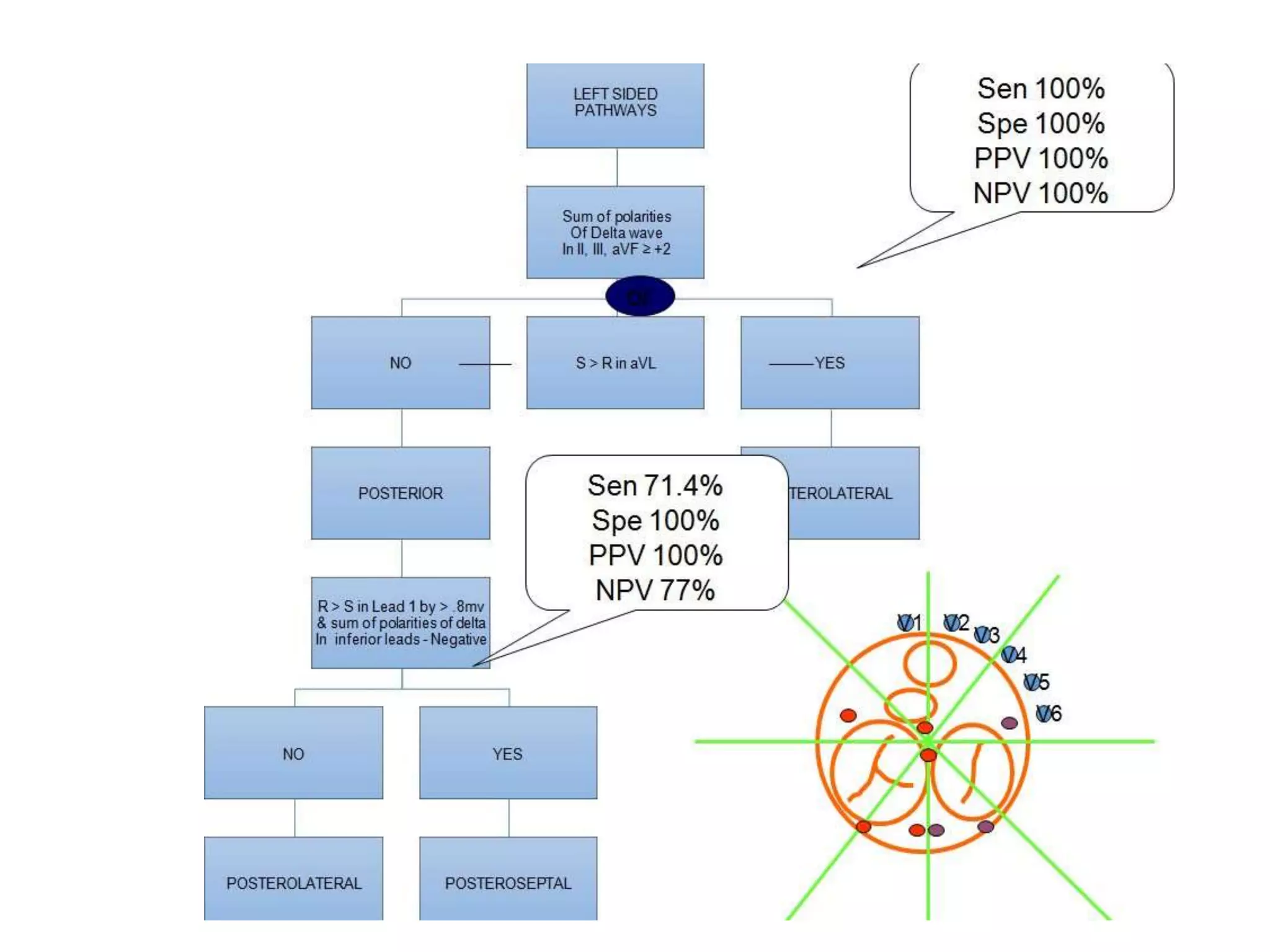
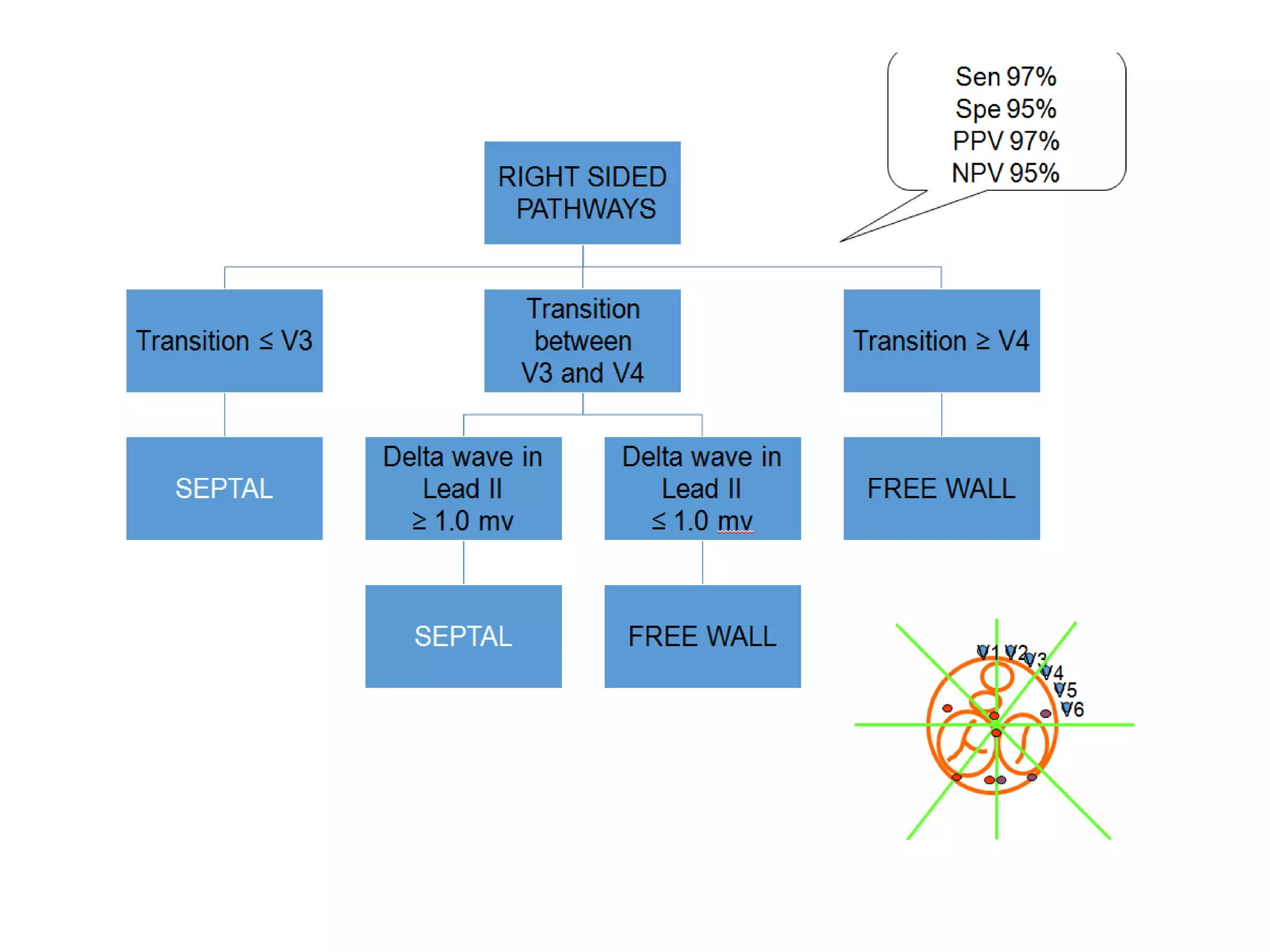
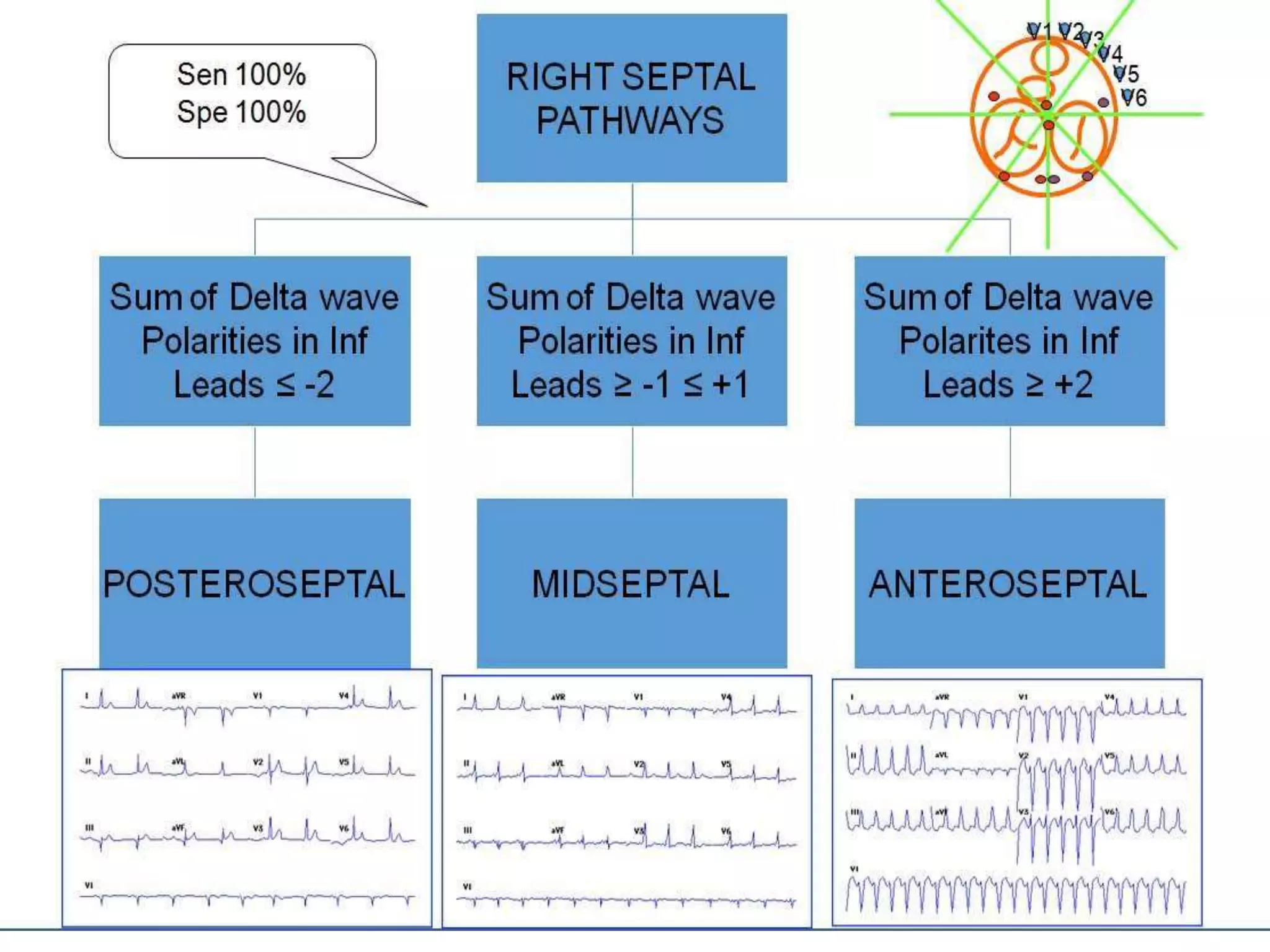
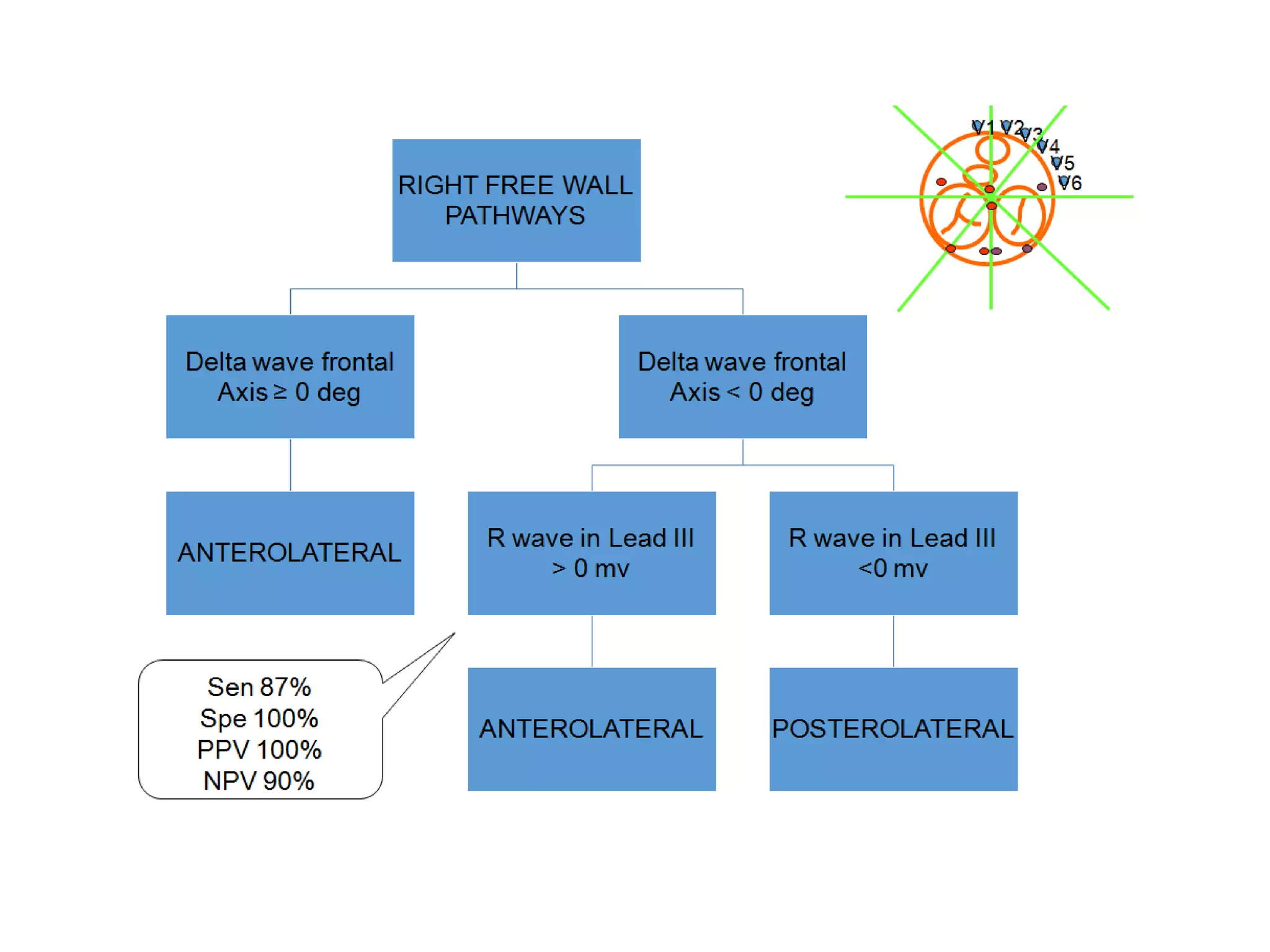
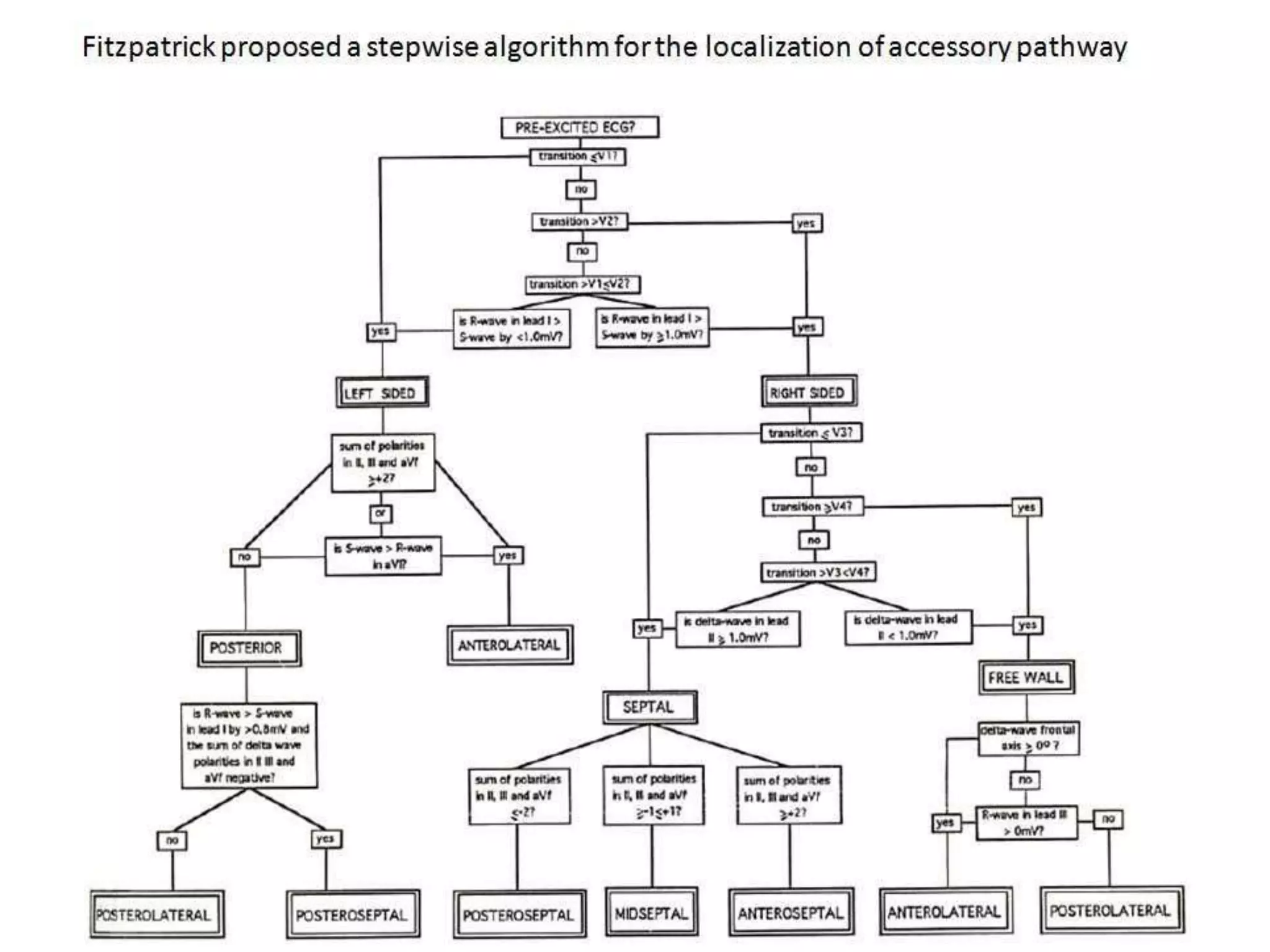
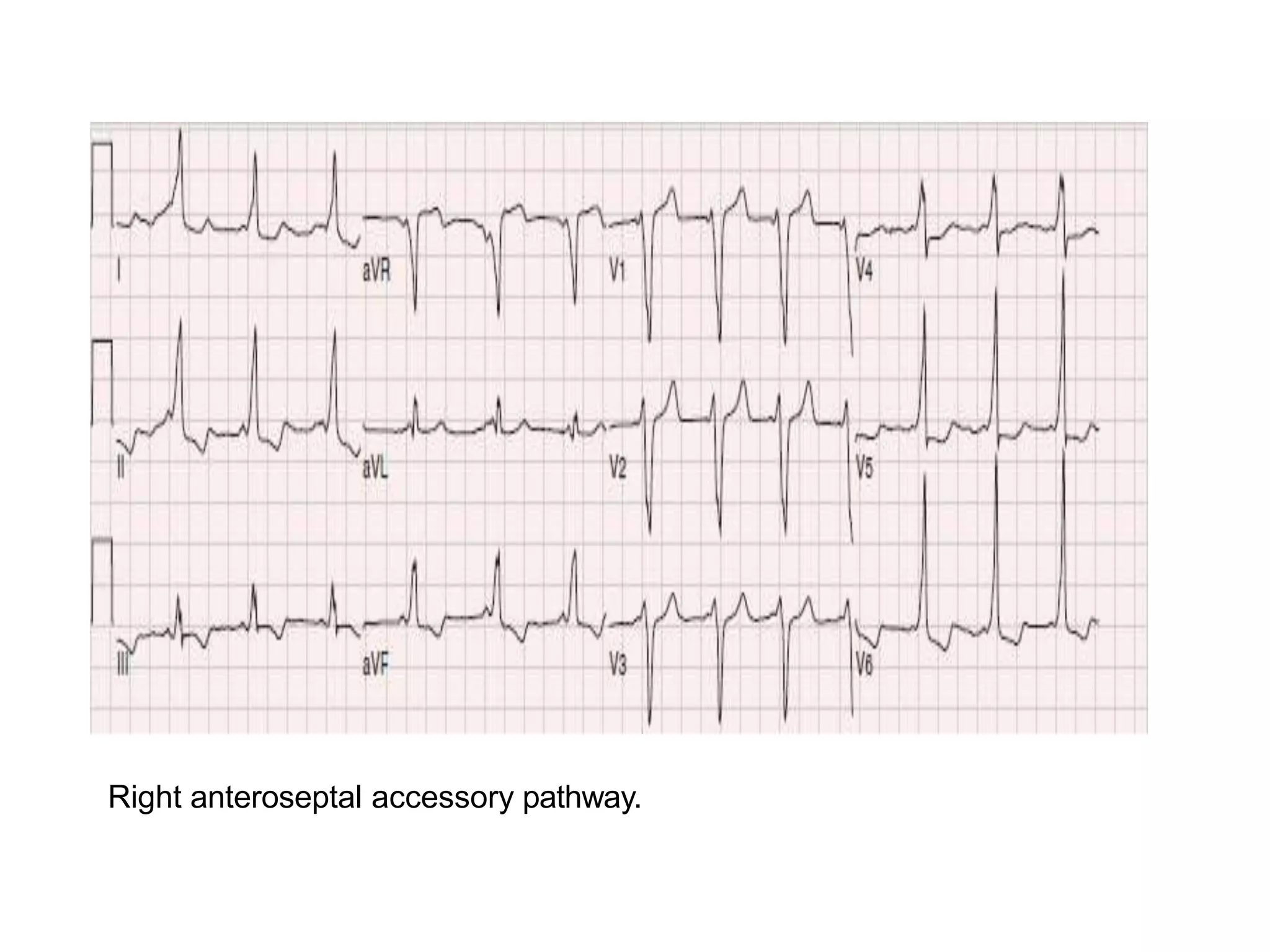
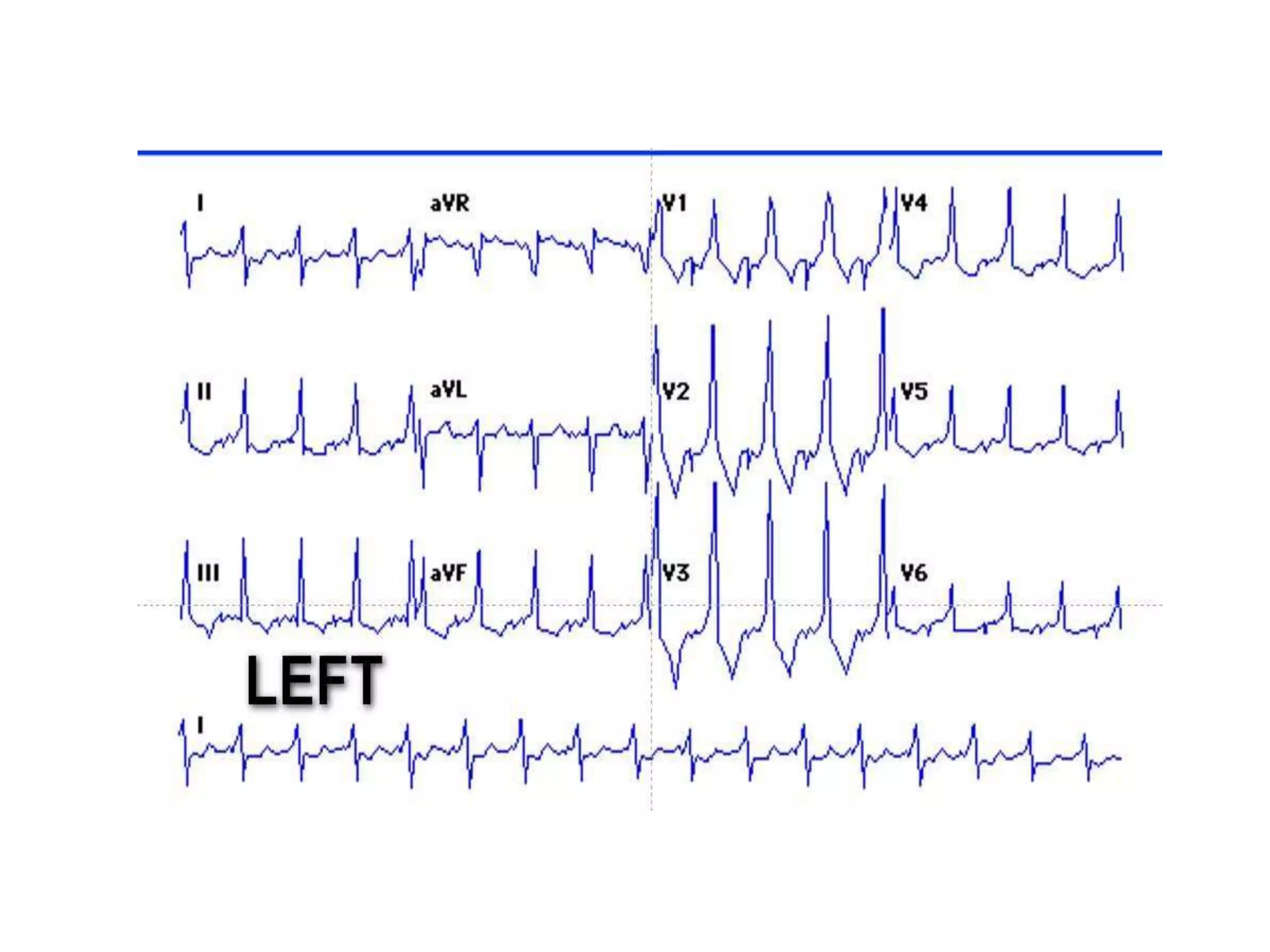
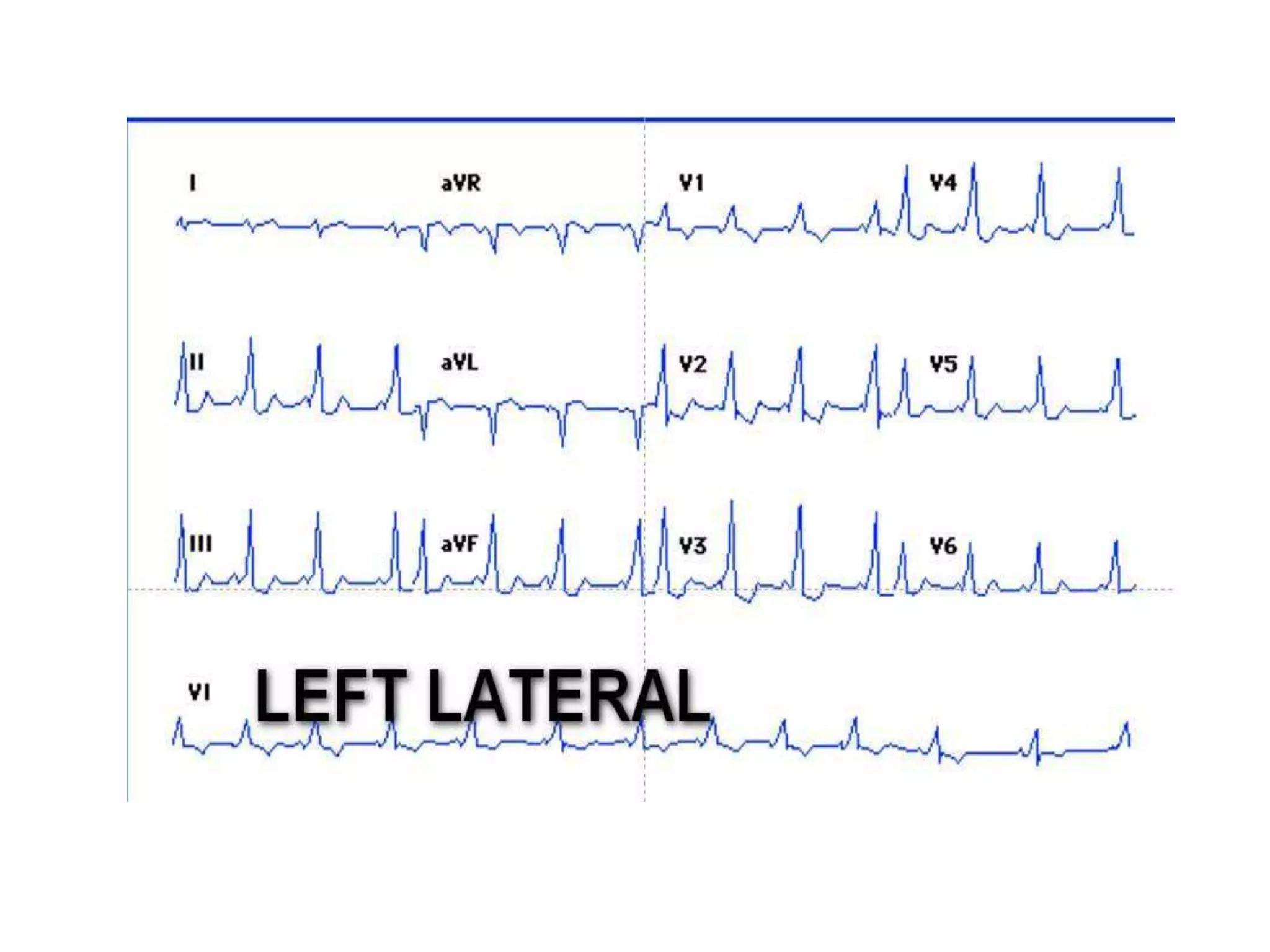
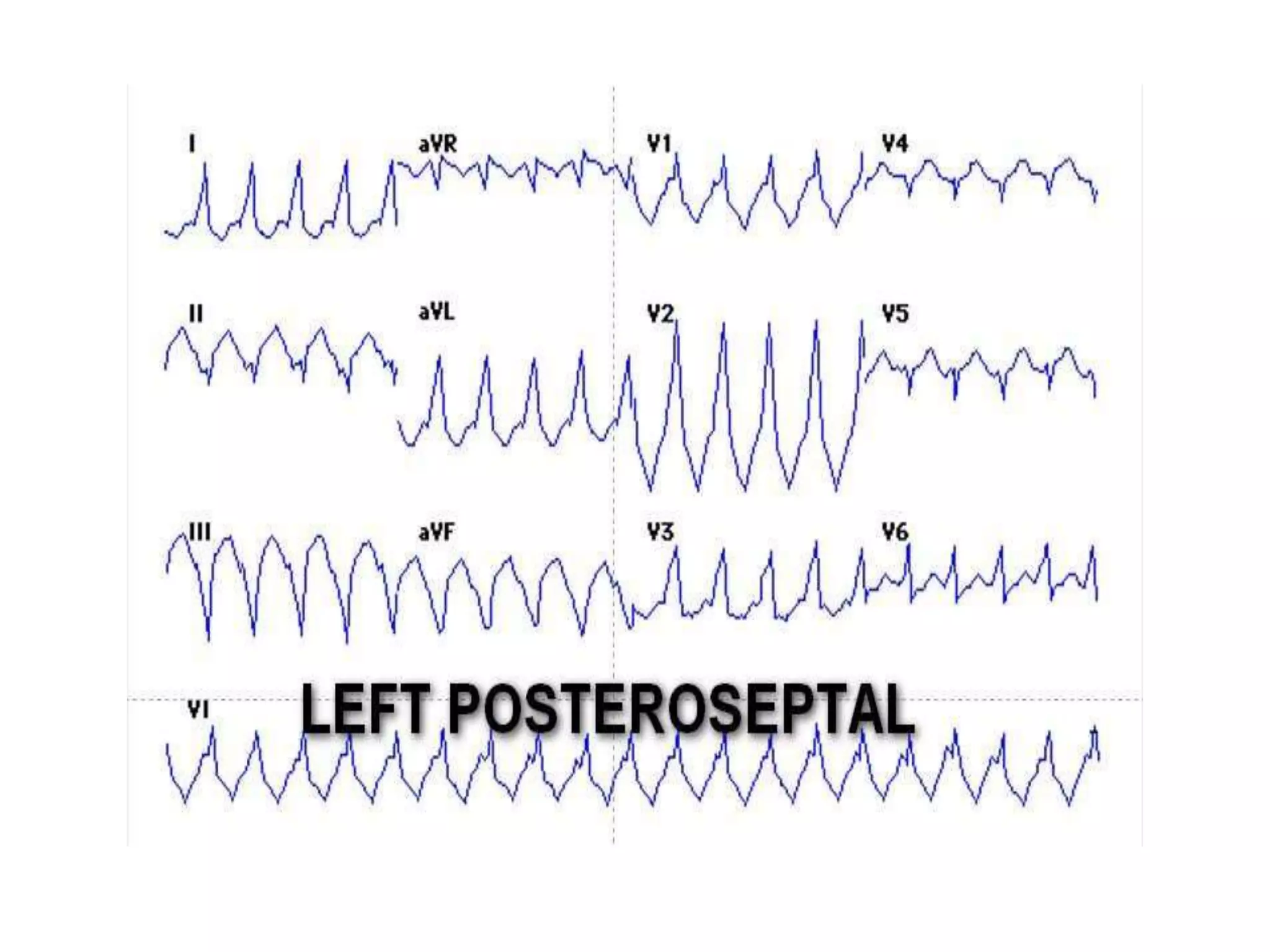
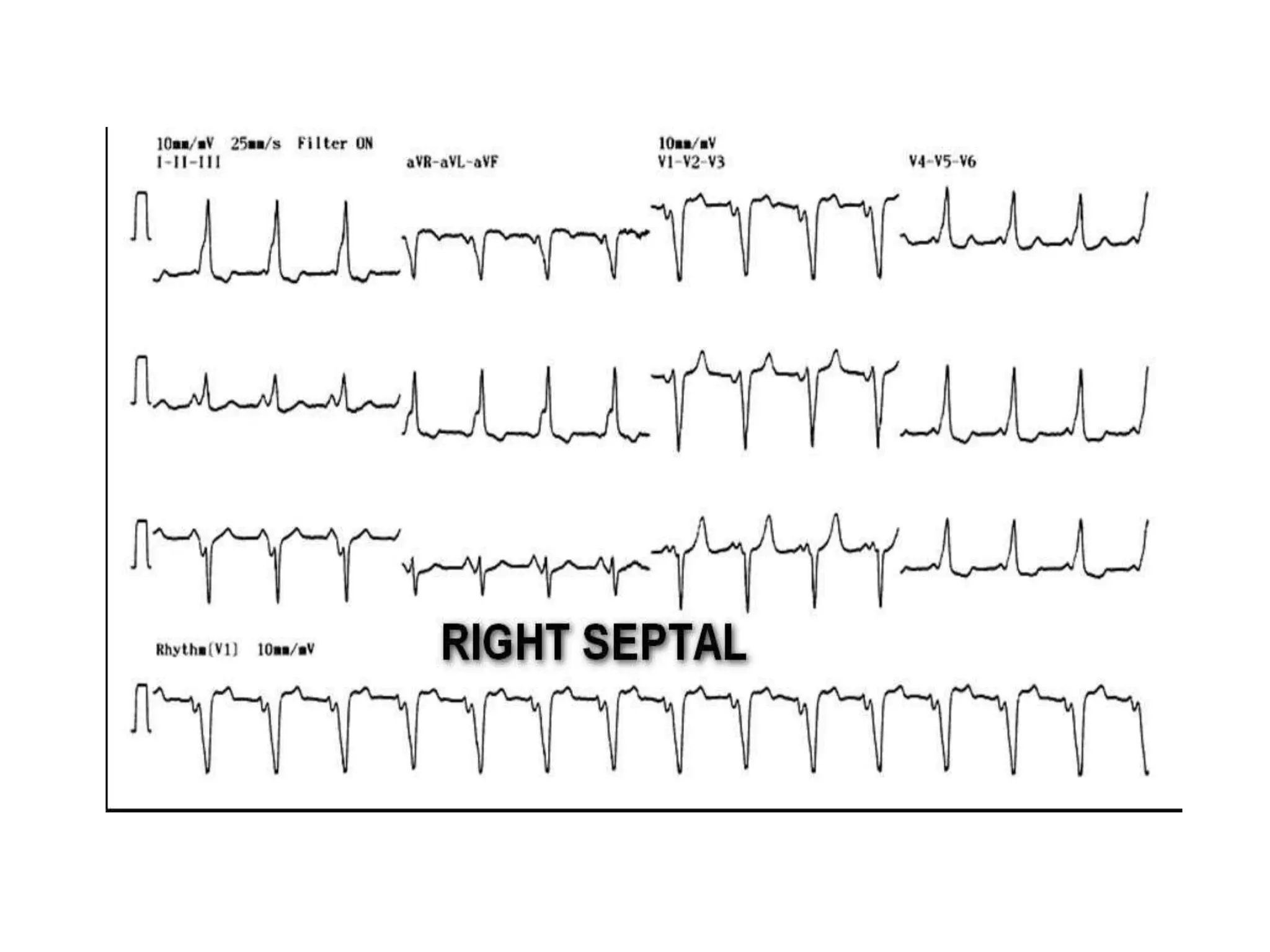
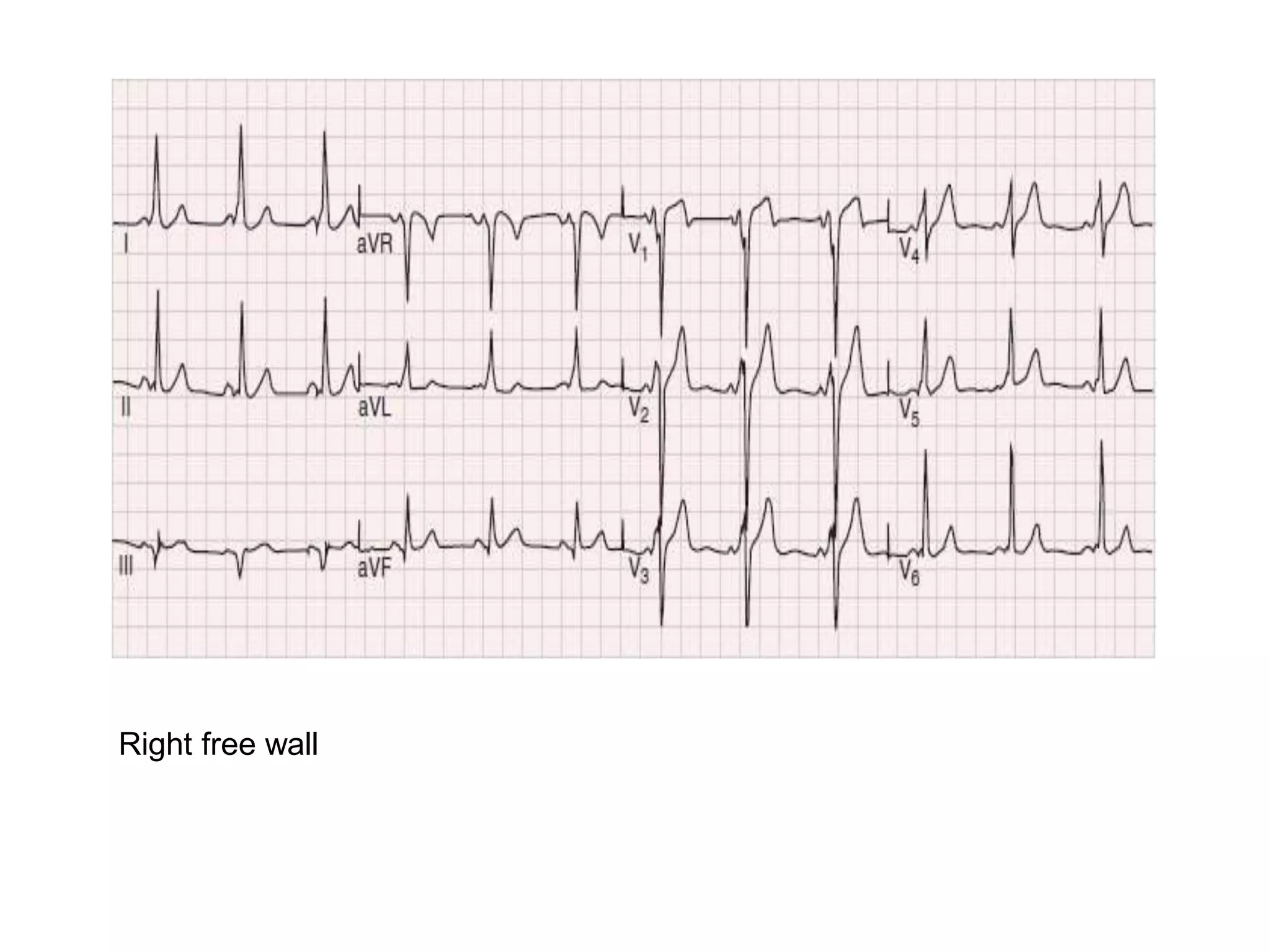
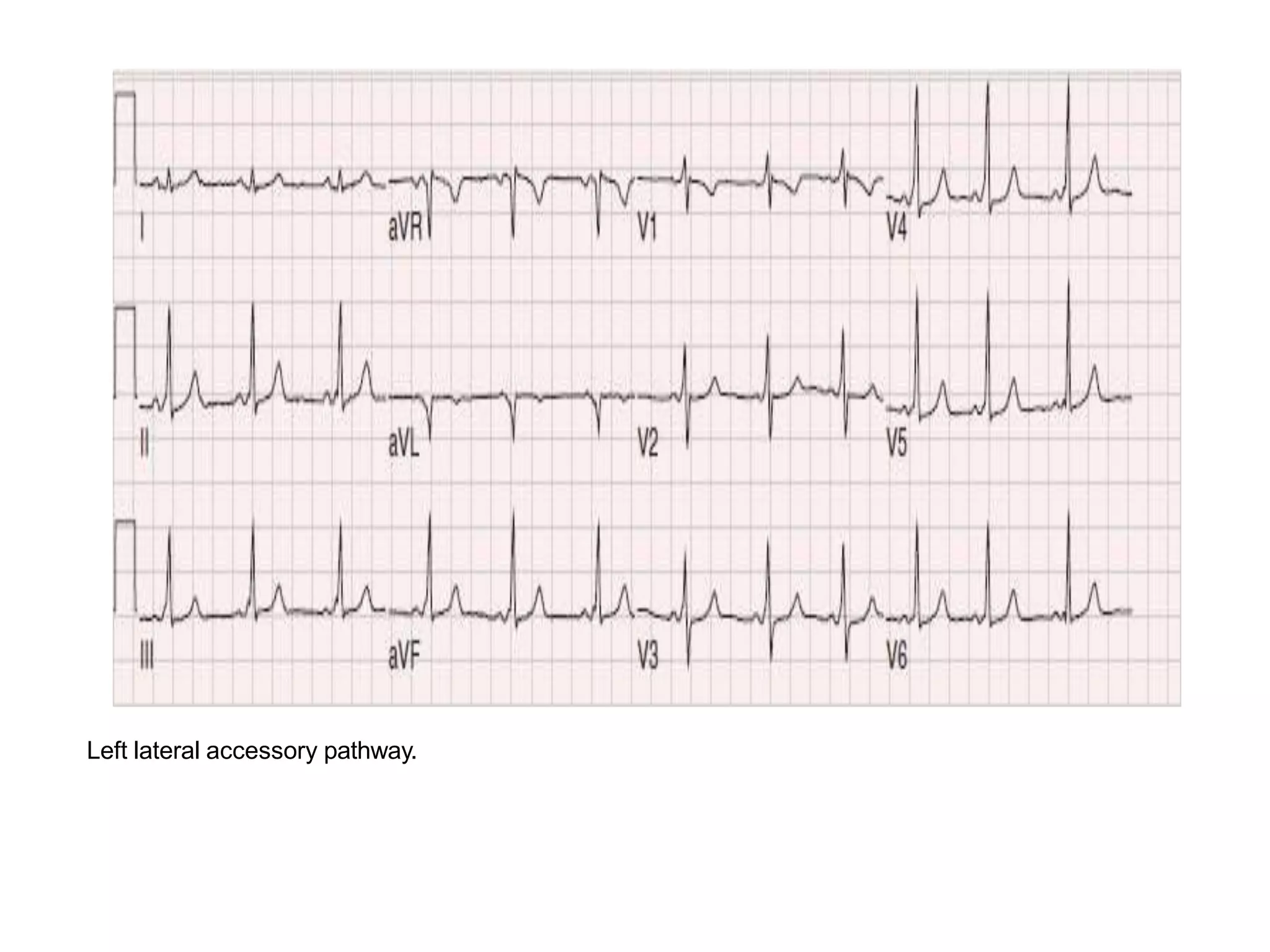
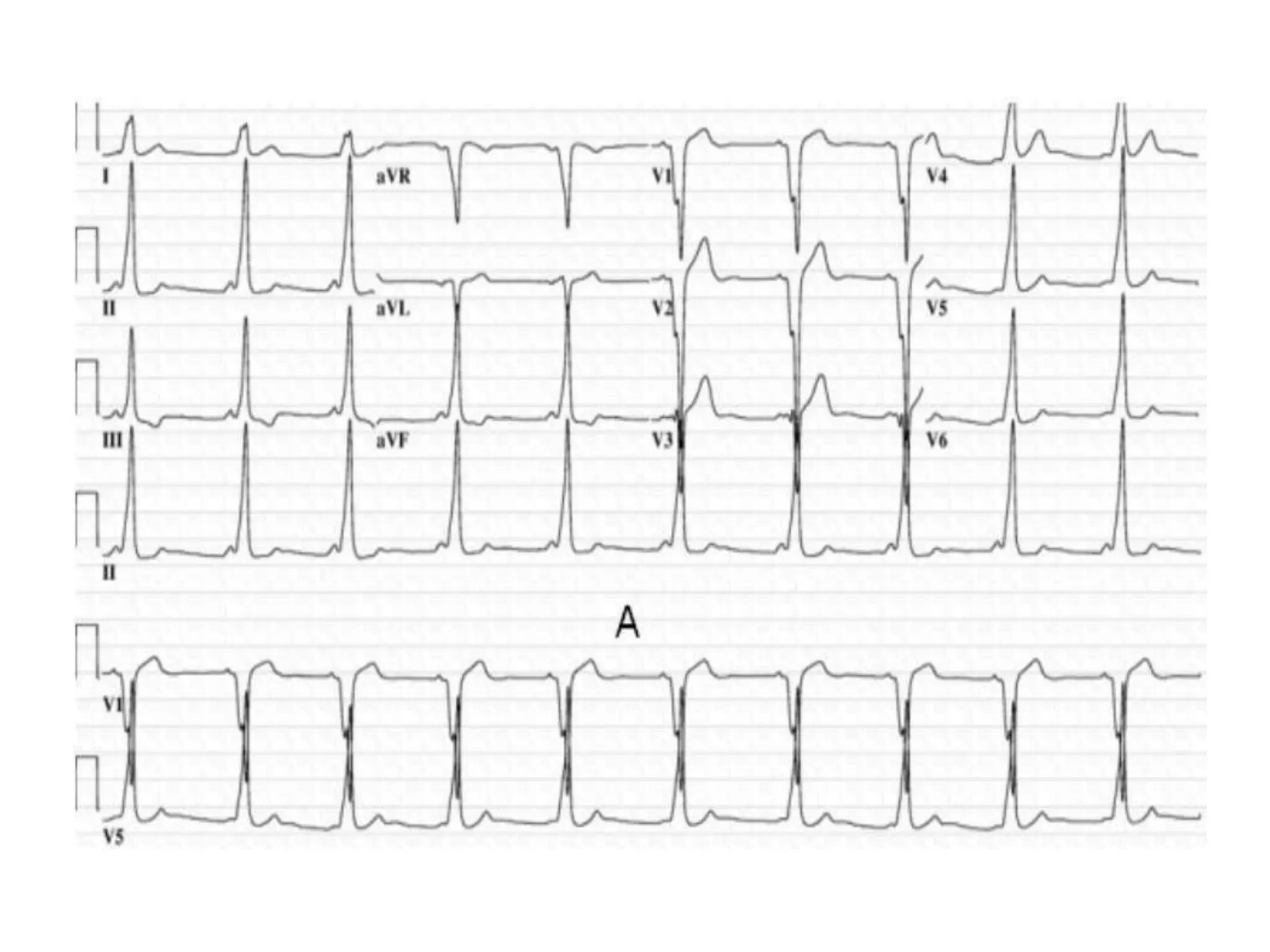
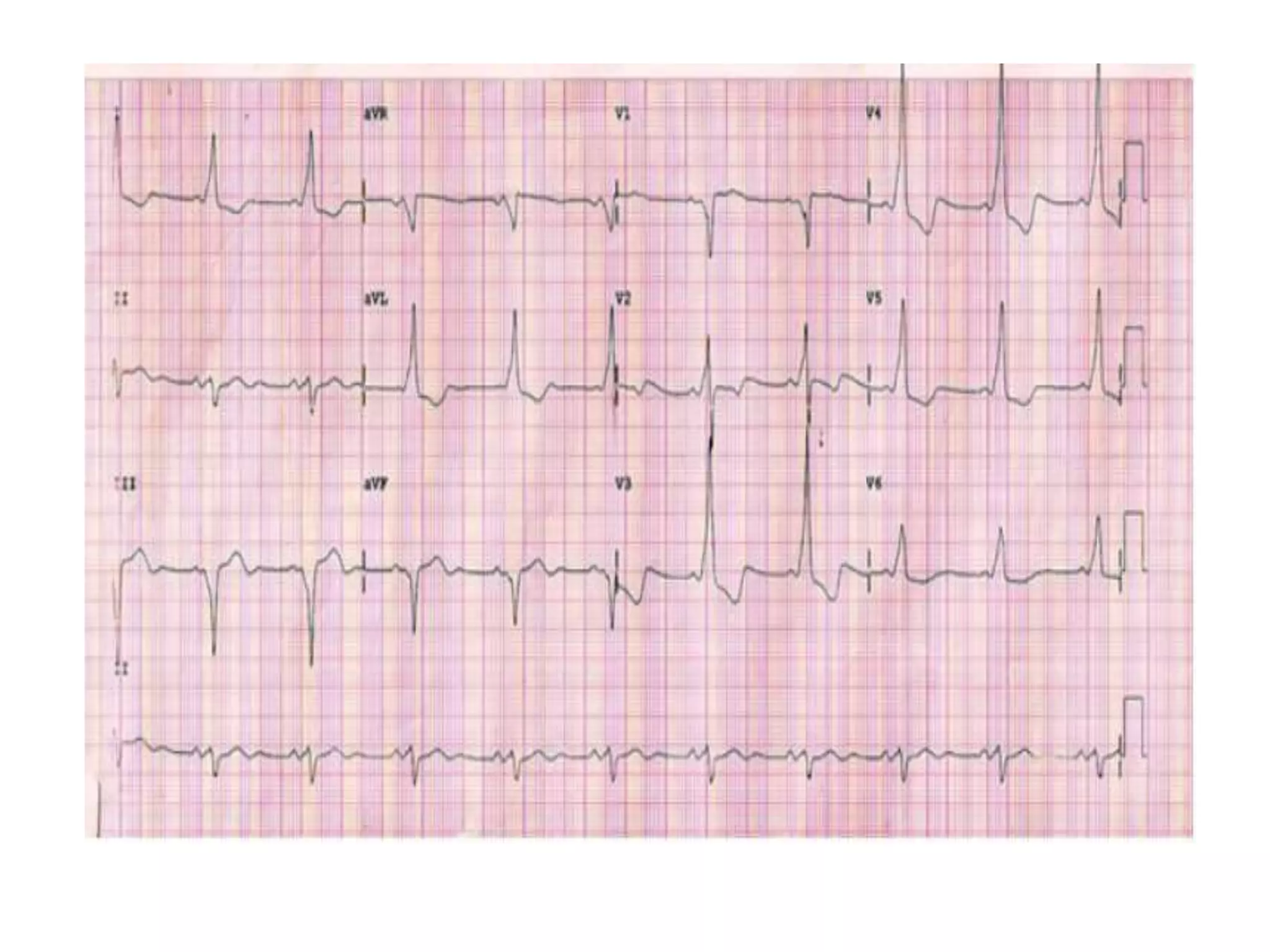
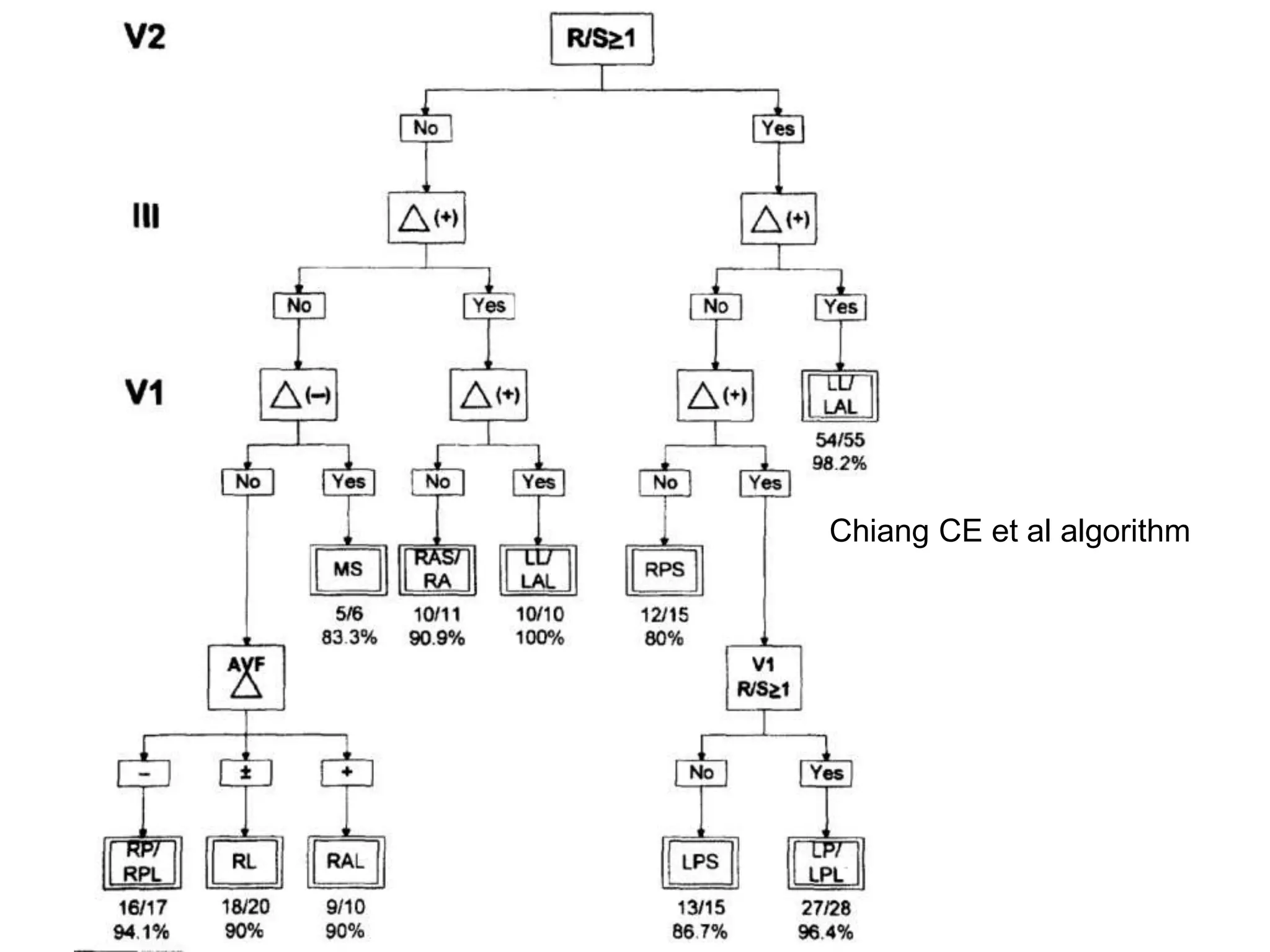
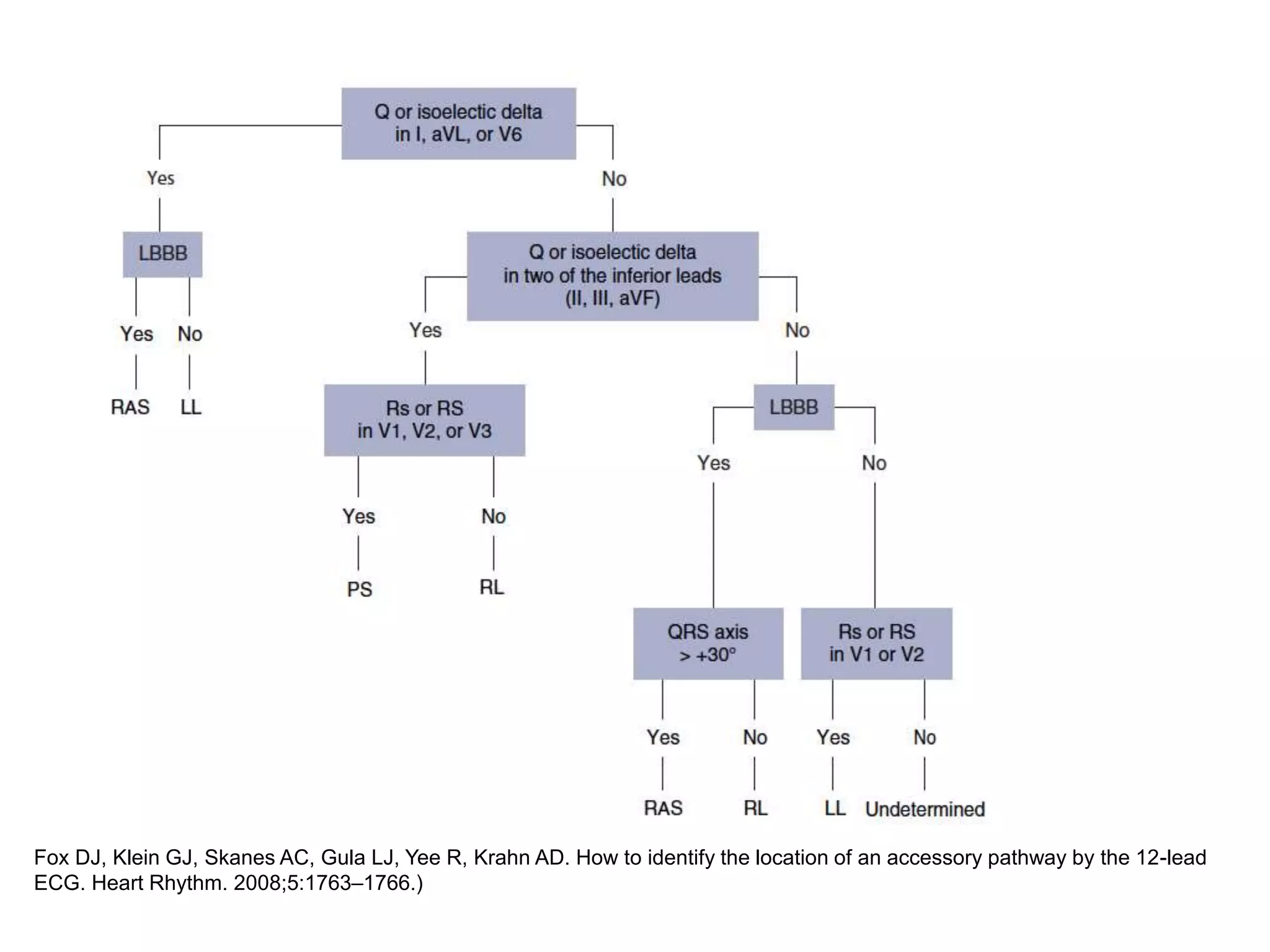
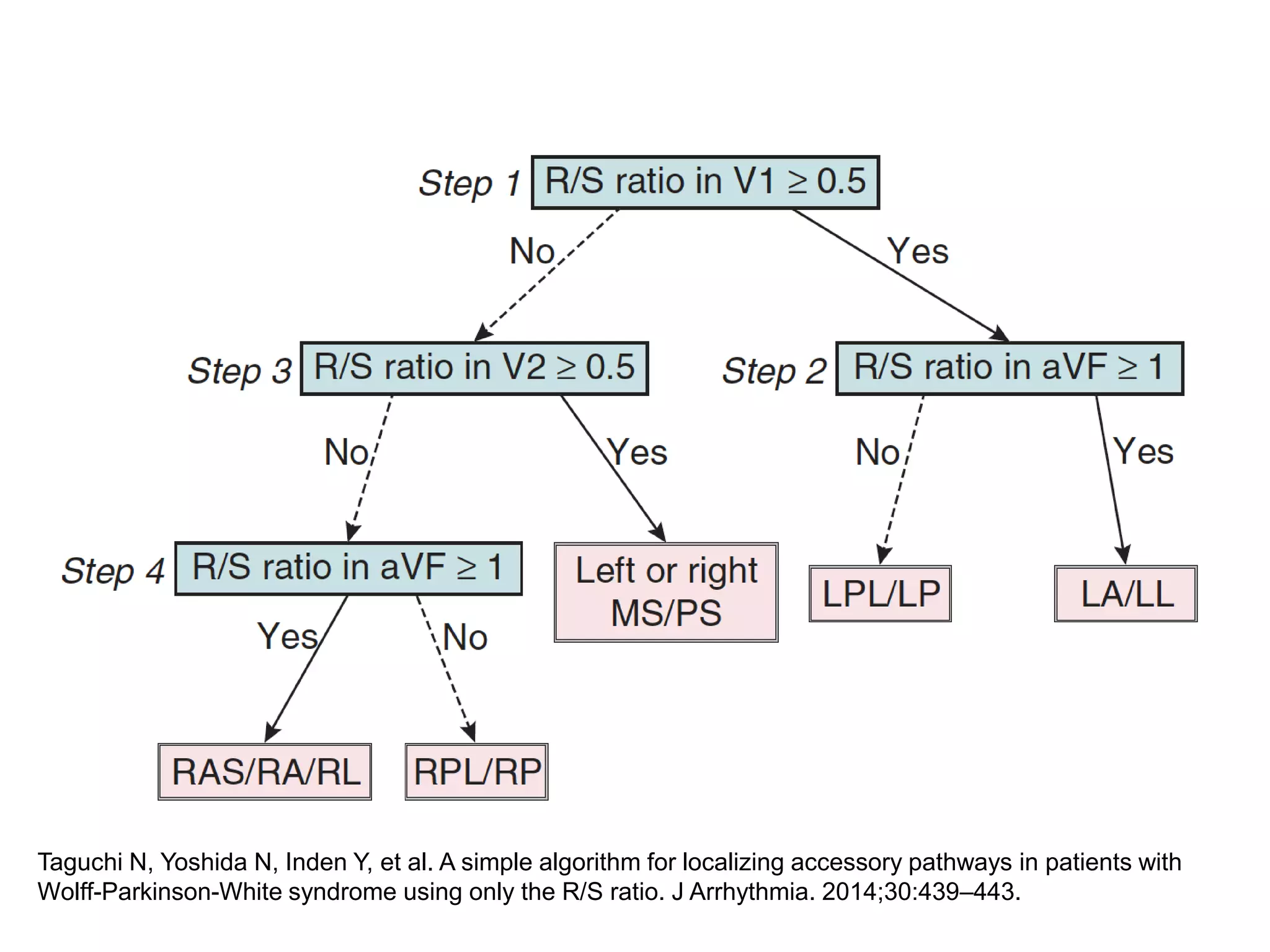
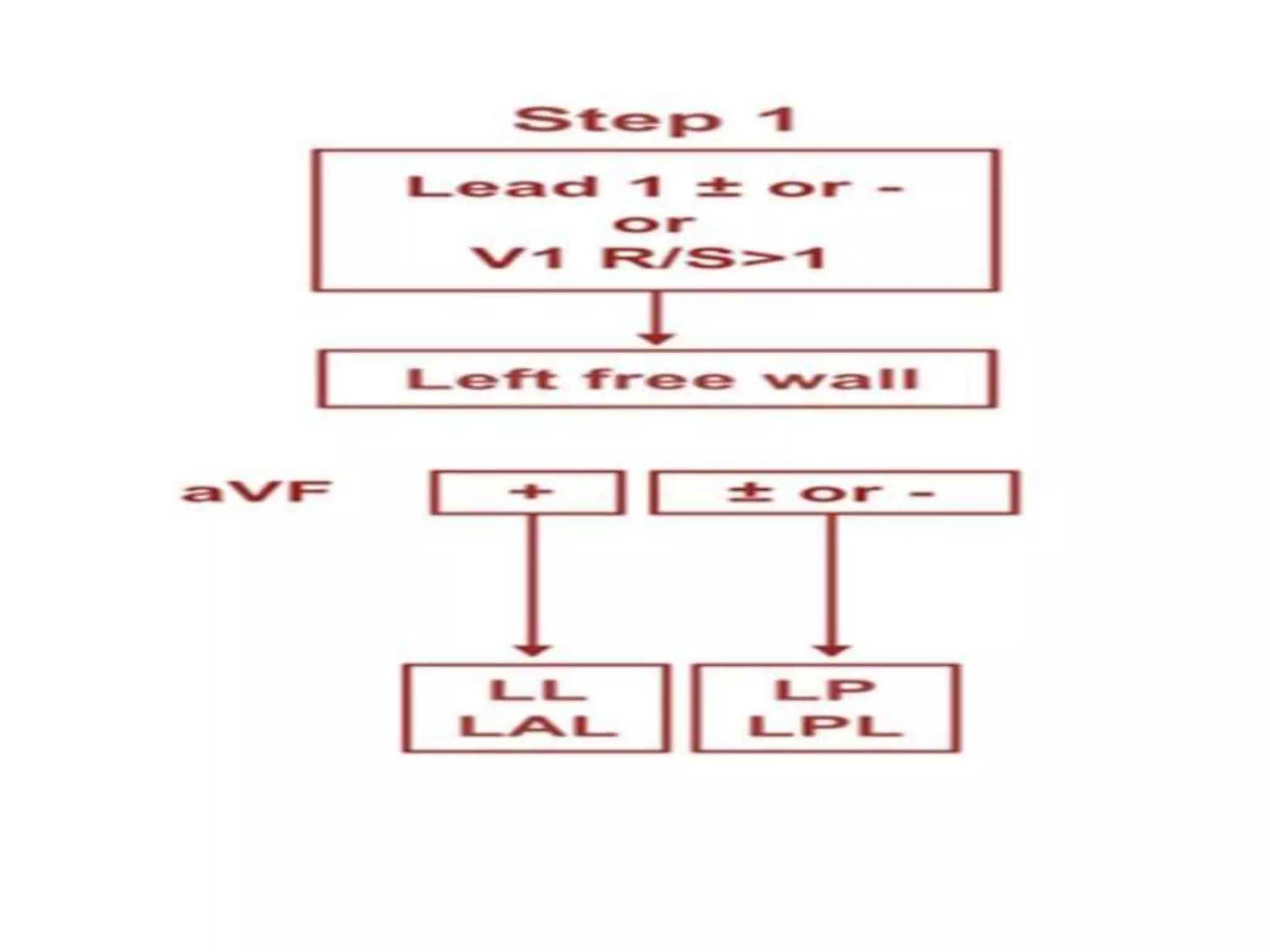
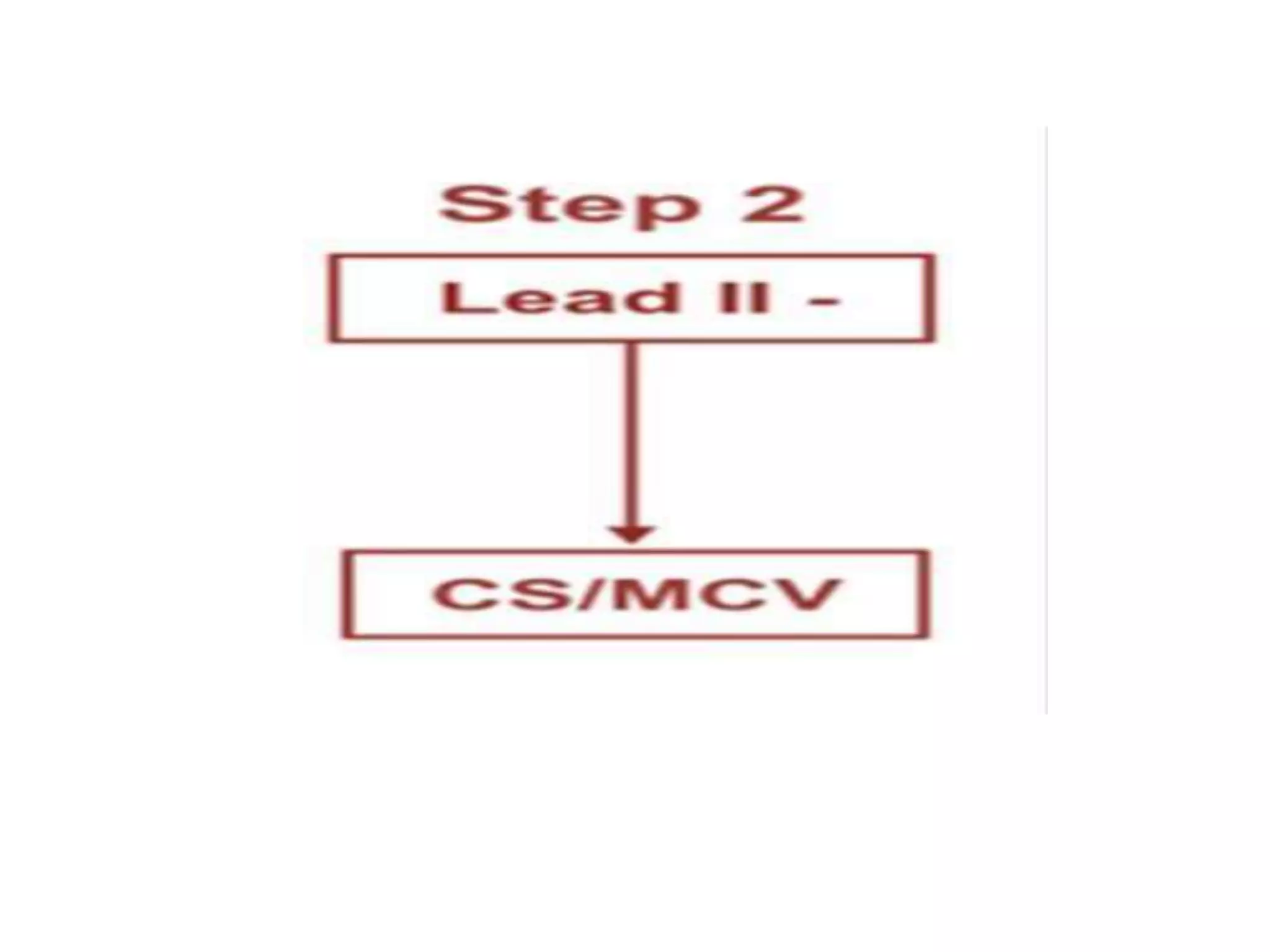
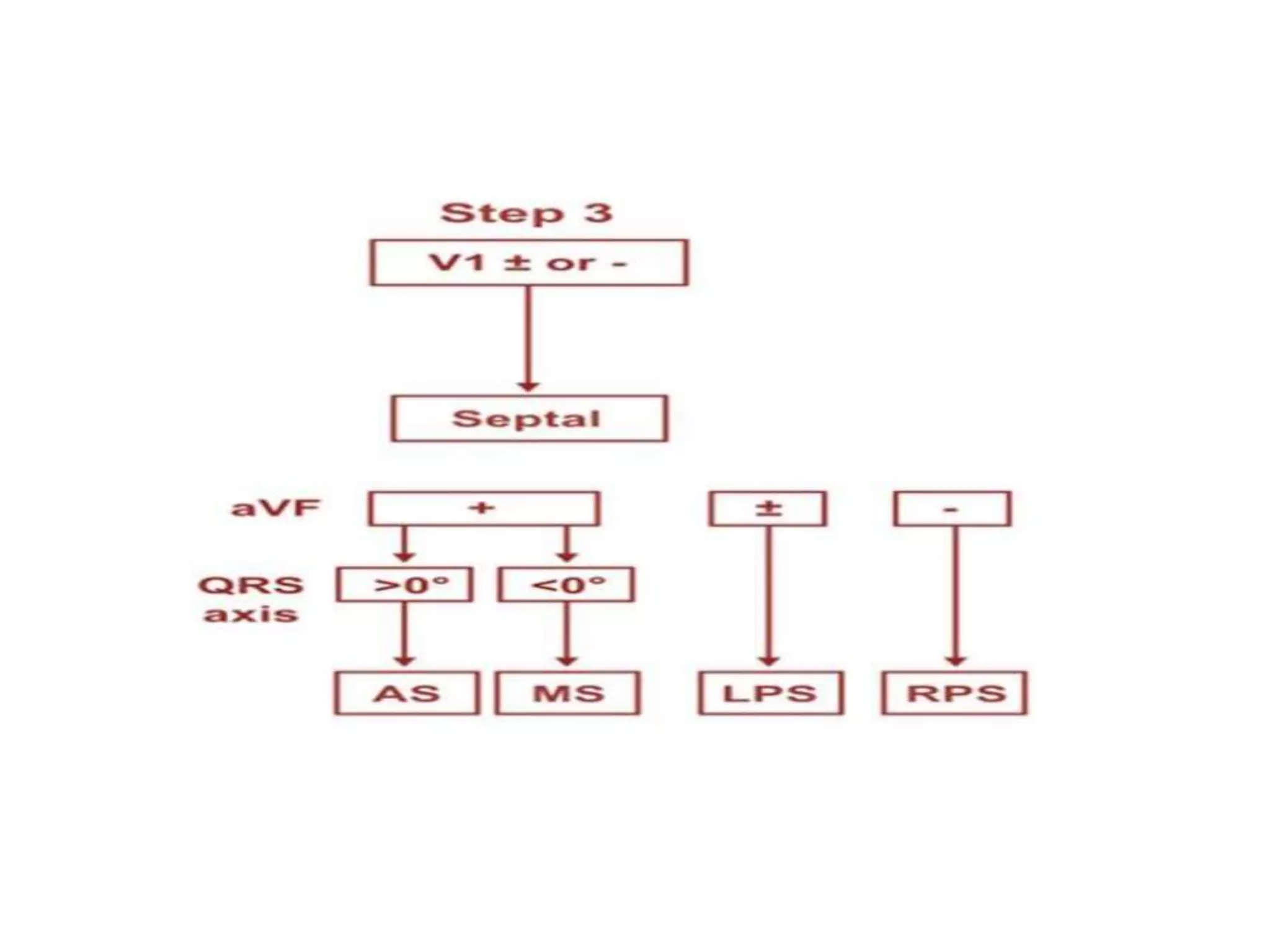
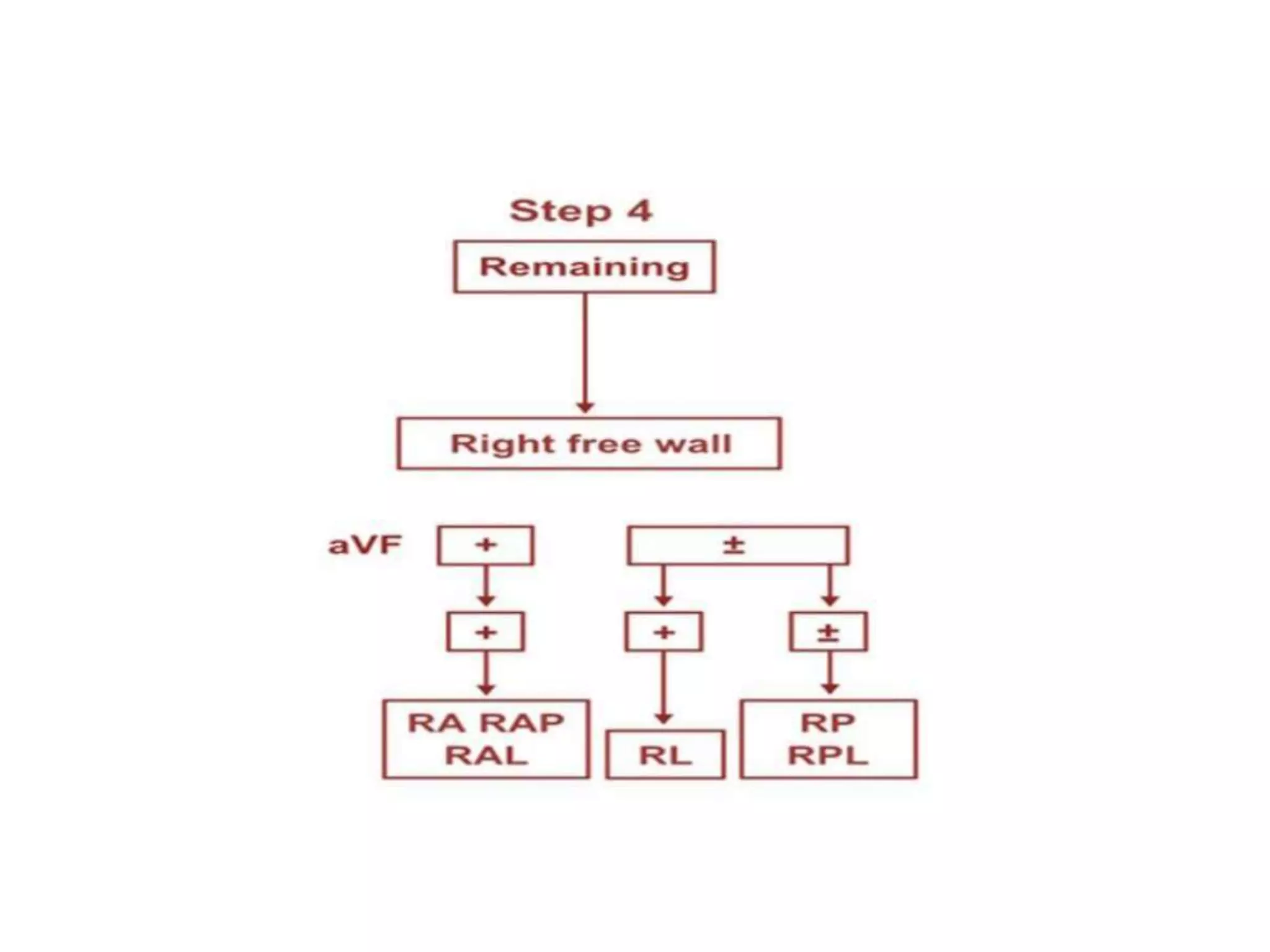
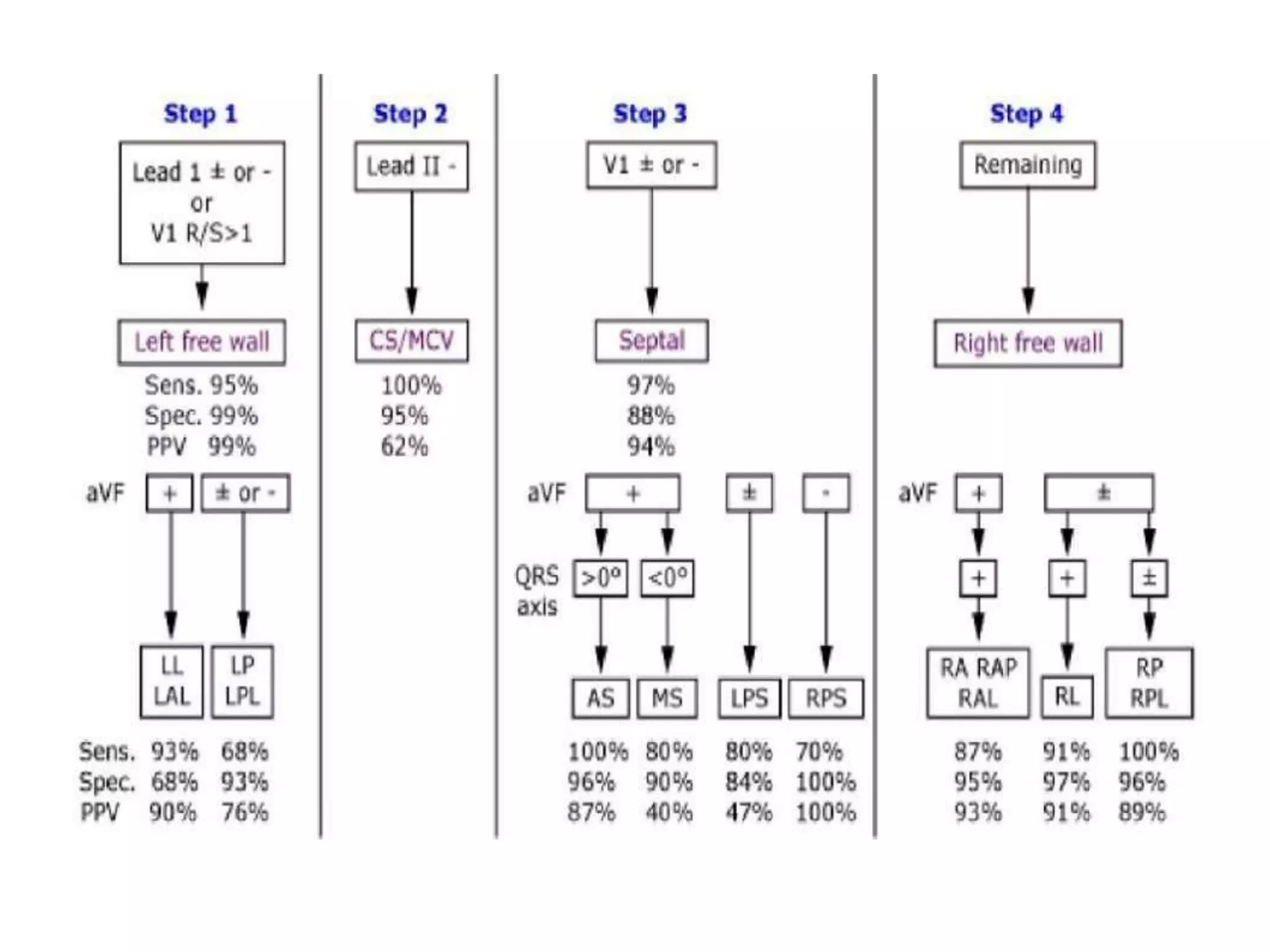
- Algorithms have been developed to predict accessory pathway location based on delta wave morphology and other ECG criteria. Fitzpatrick's algorithm divides pathways into 8 anatomical locations.
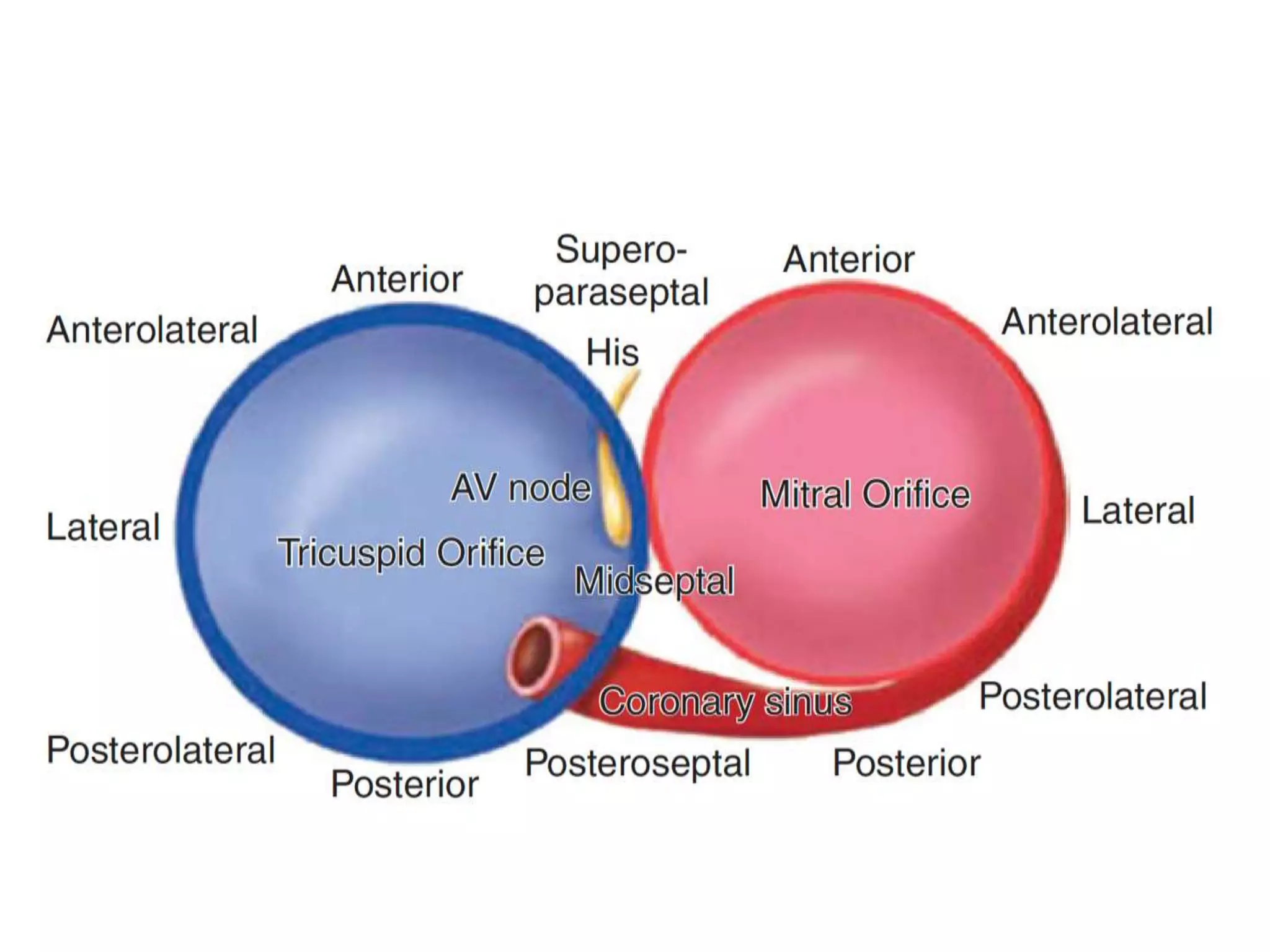
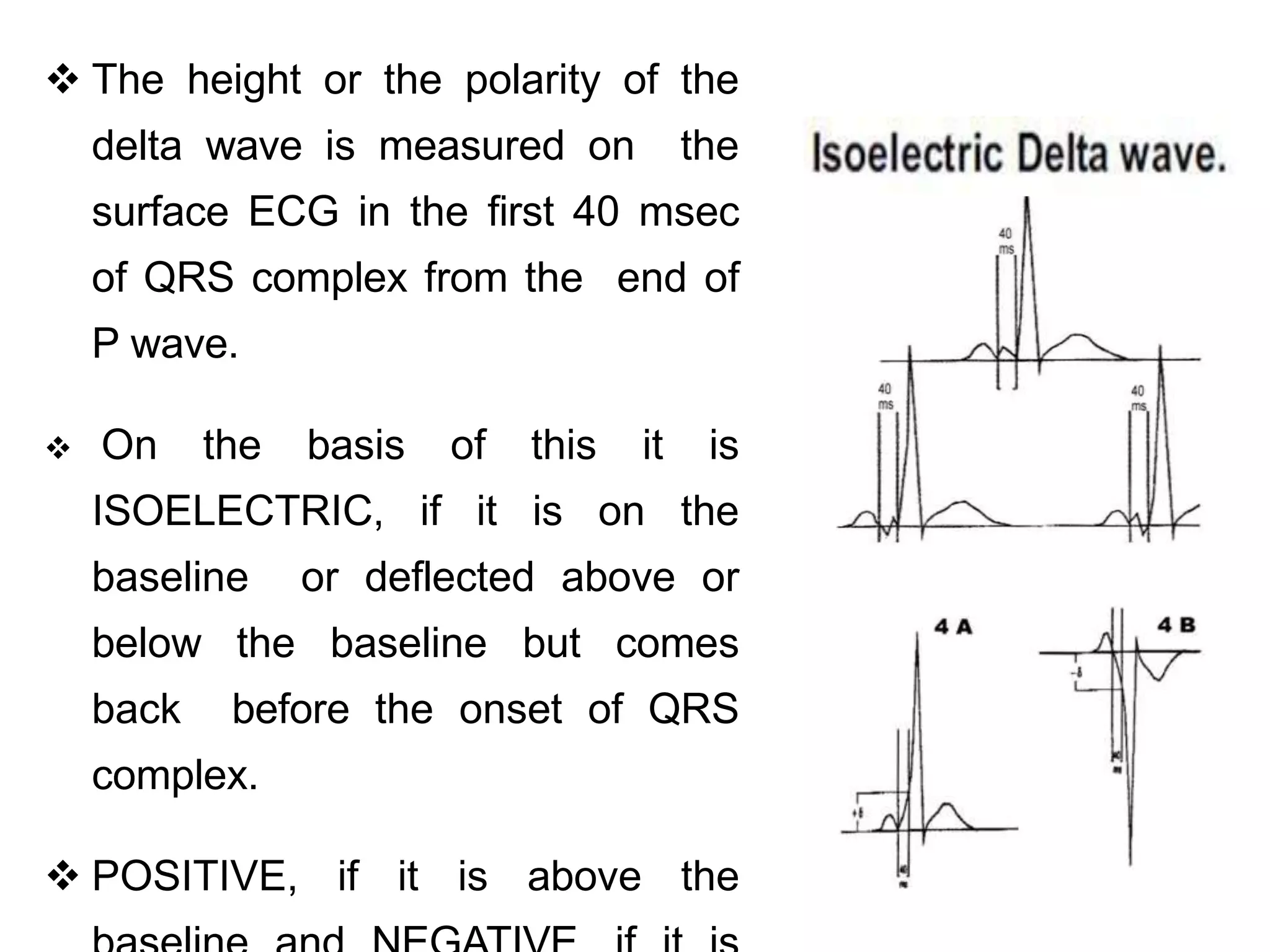
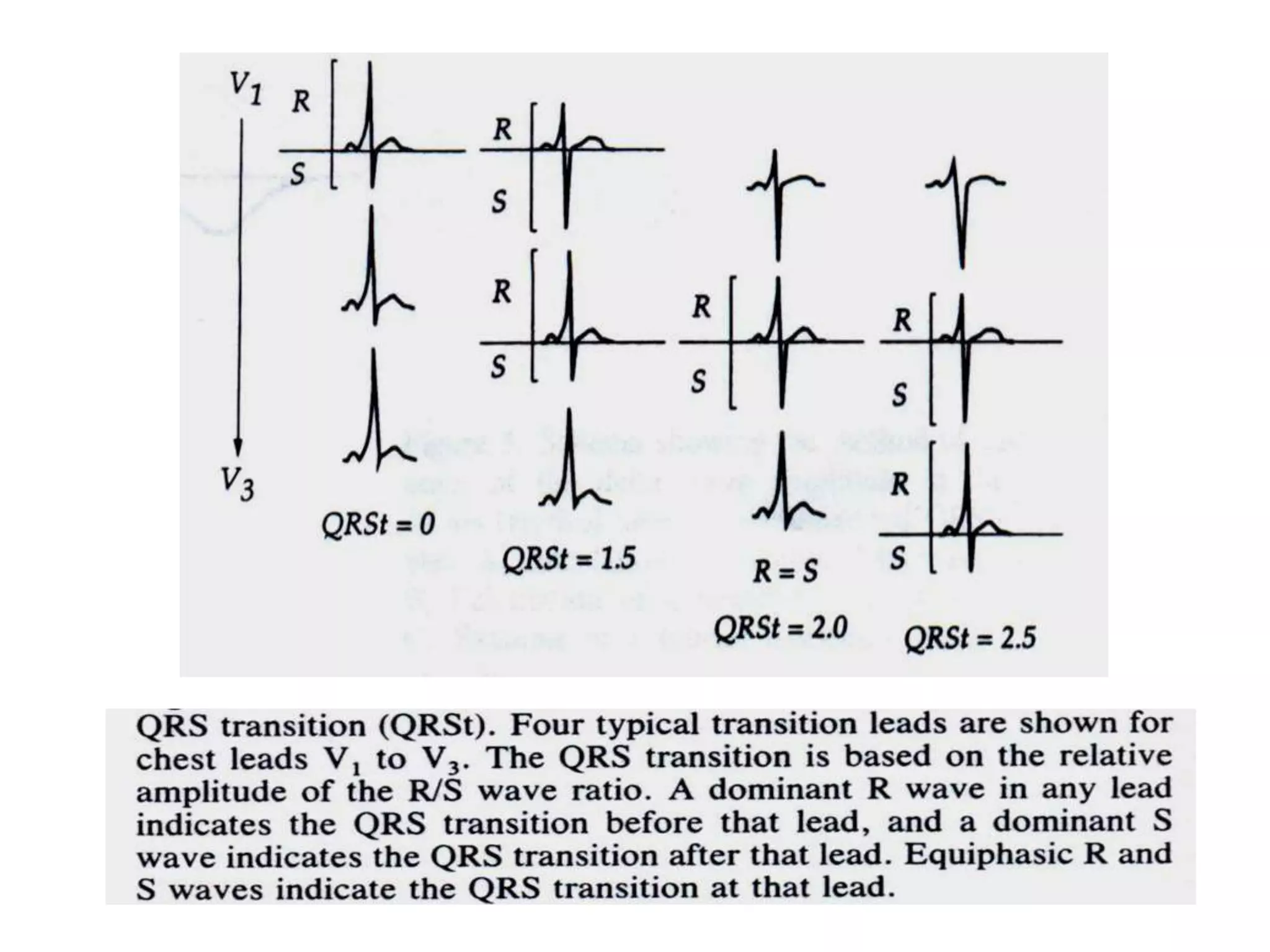
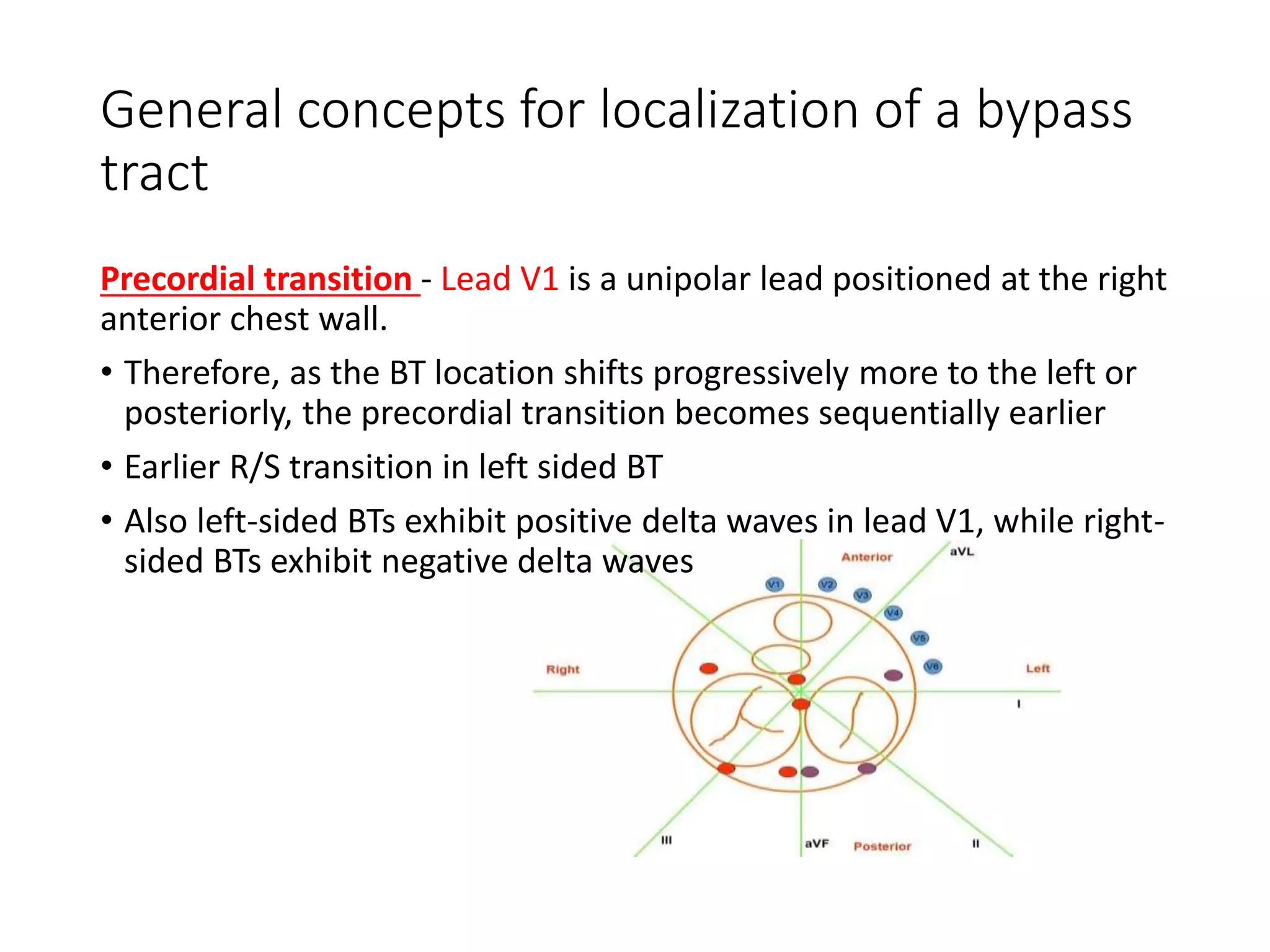
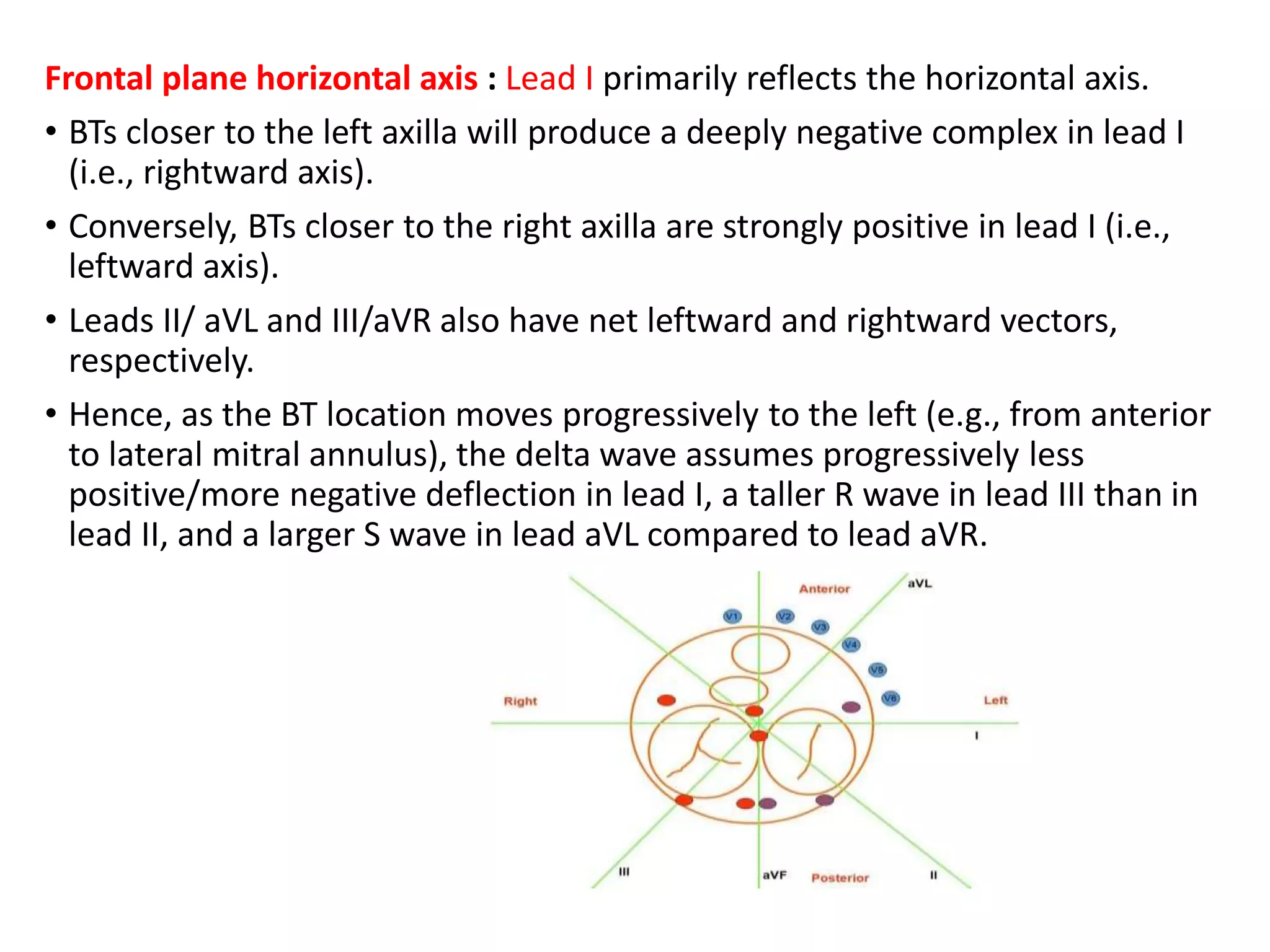
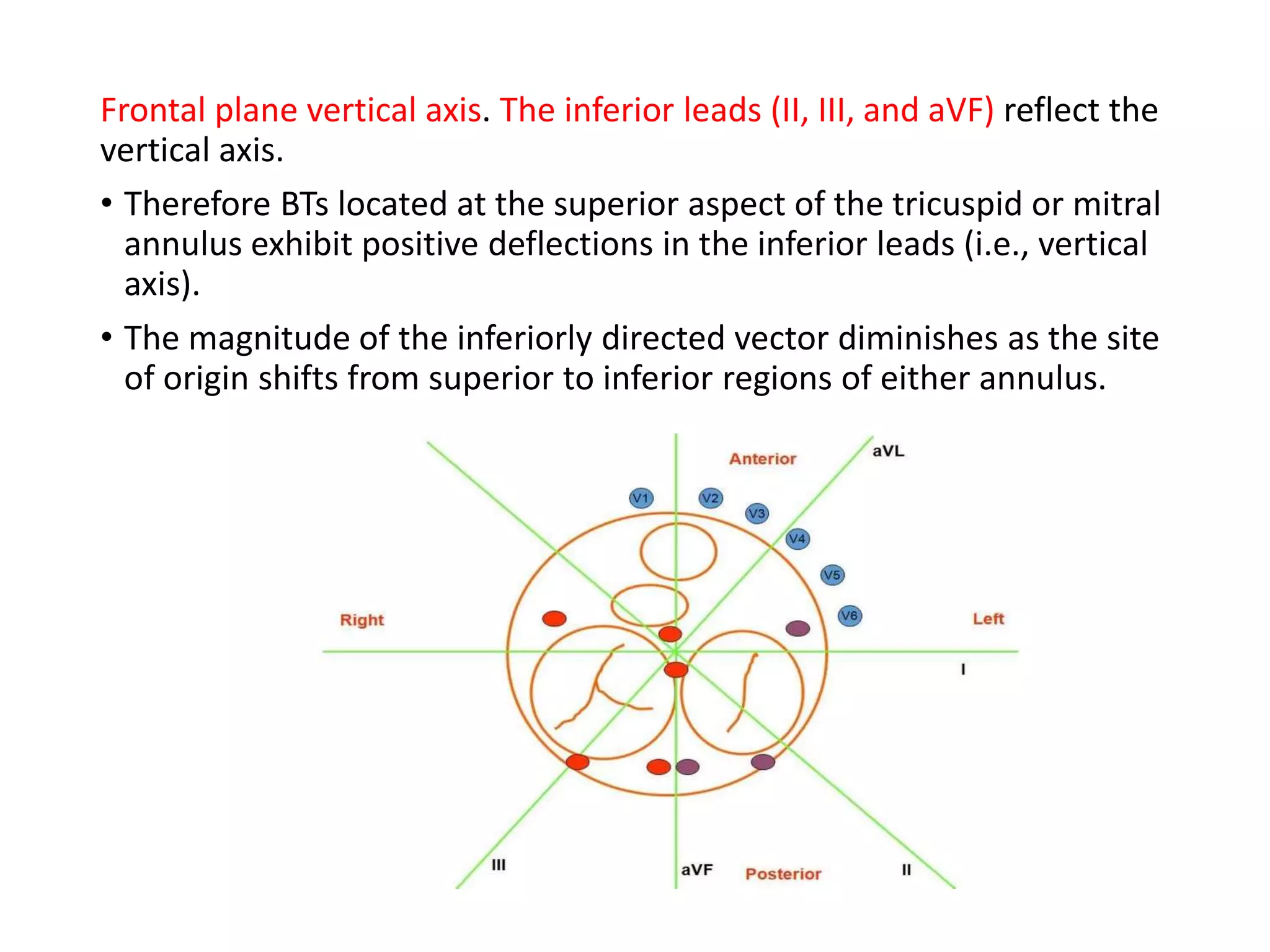
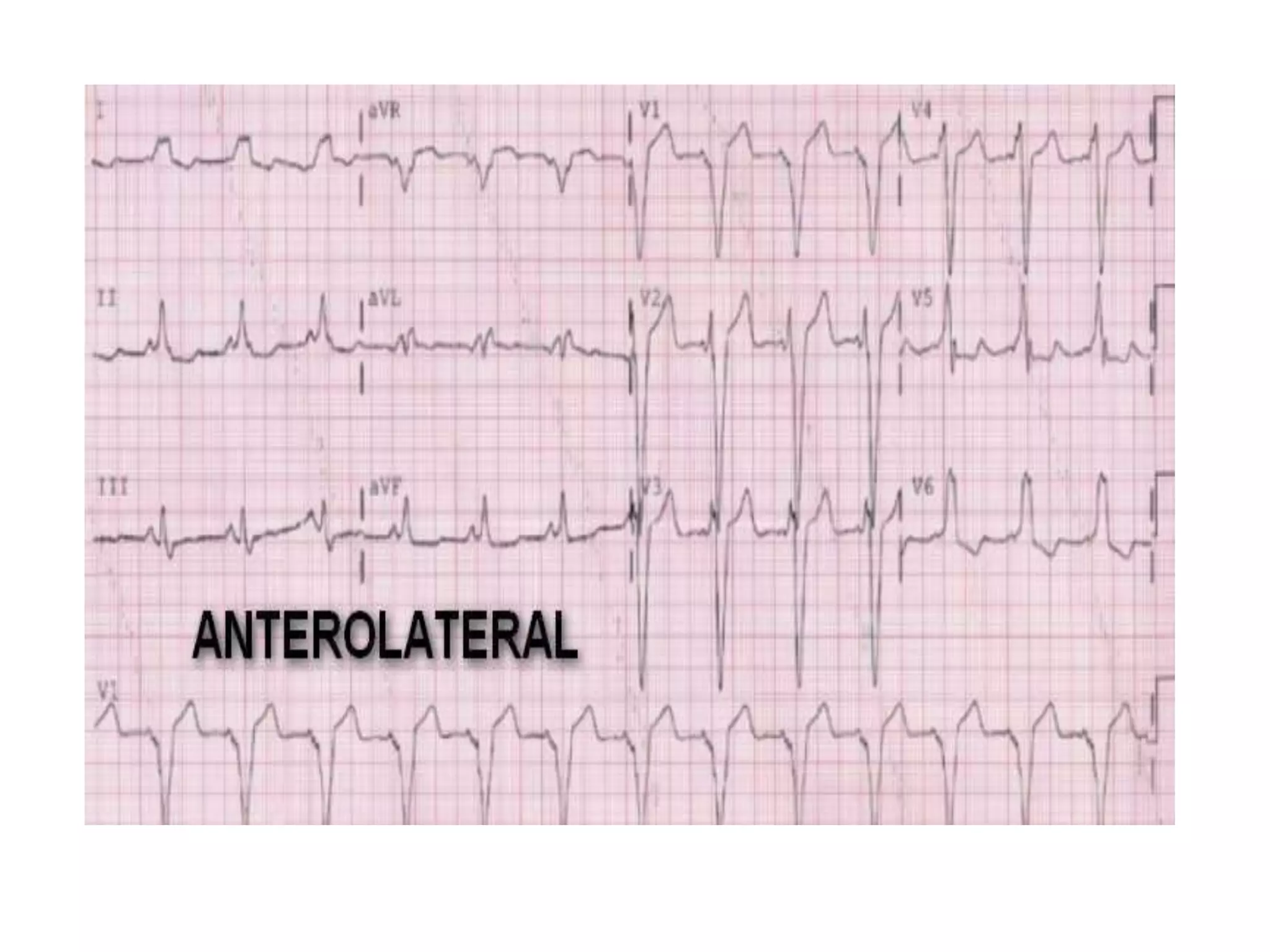
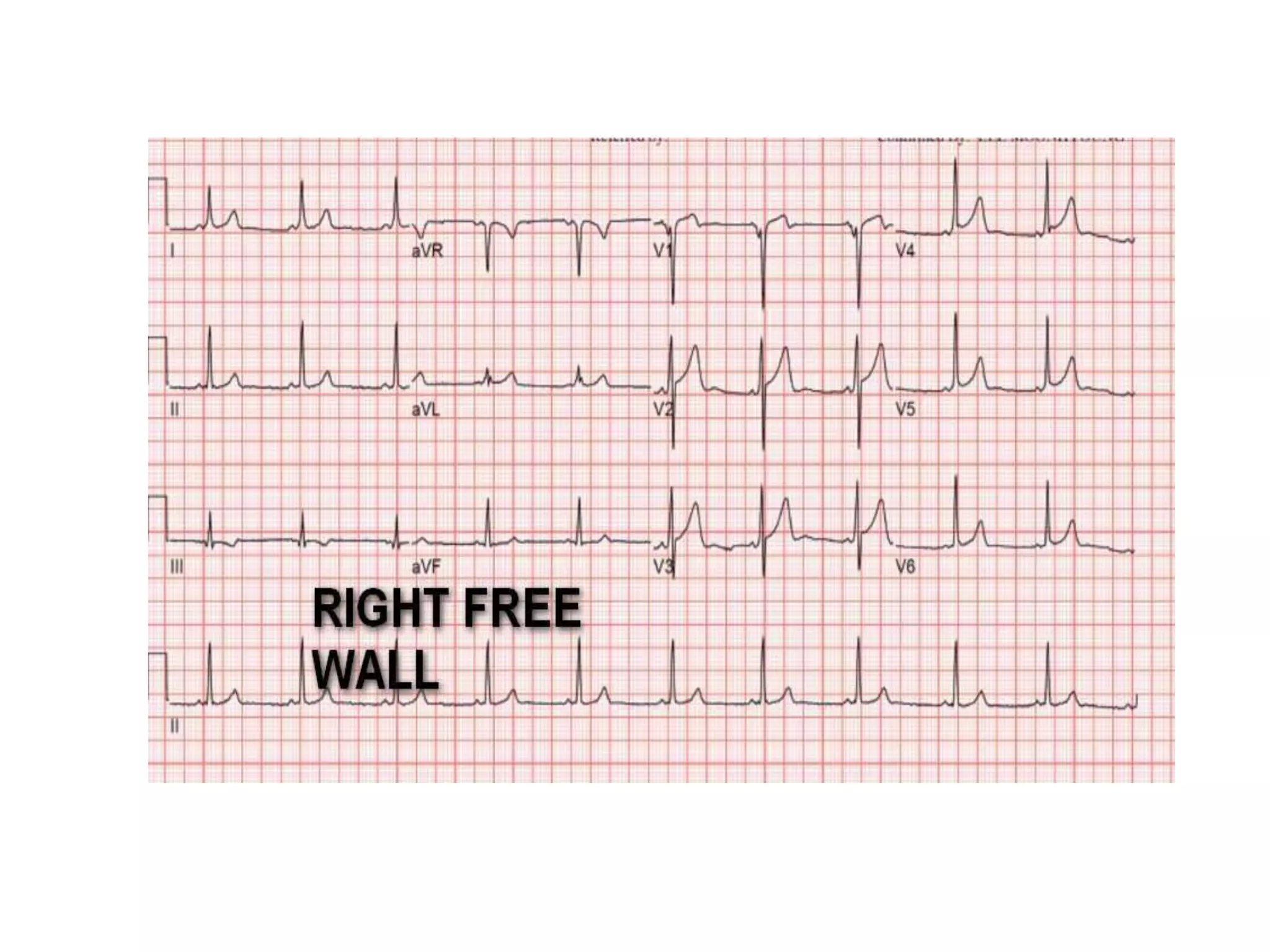
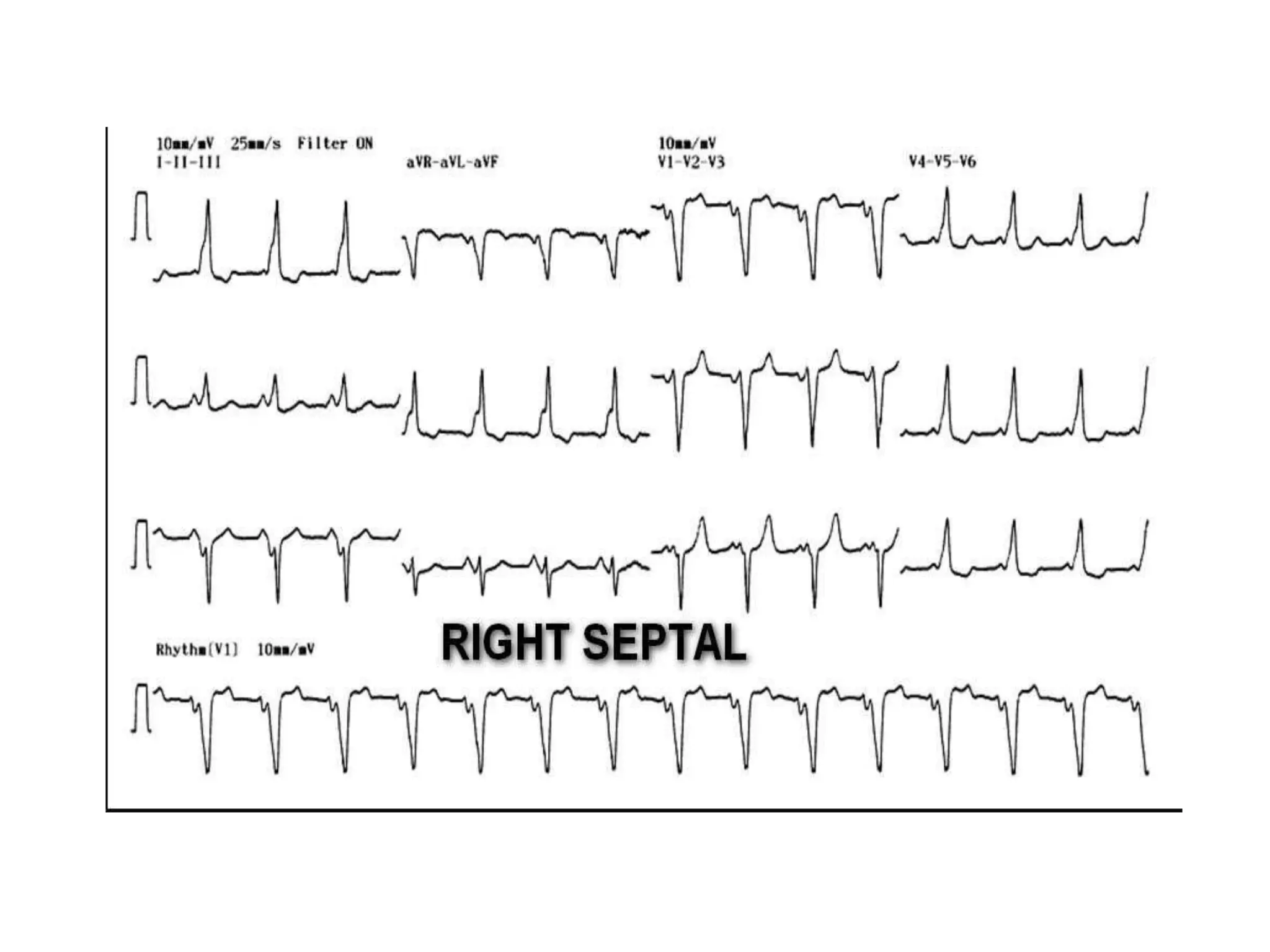
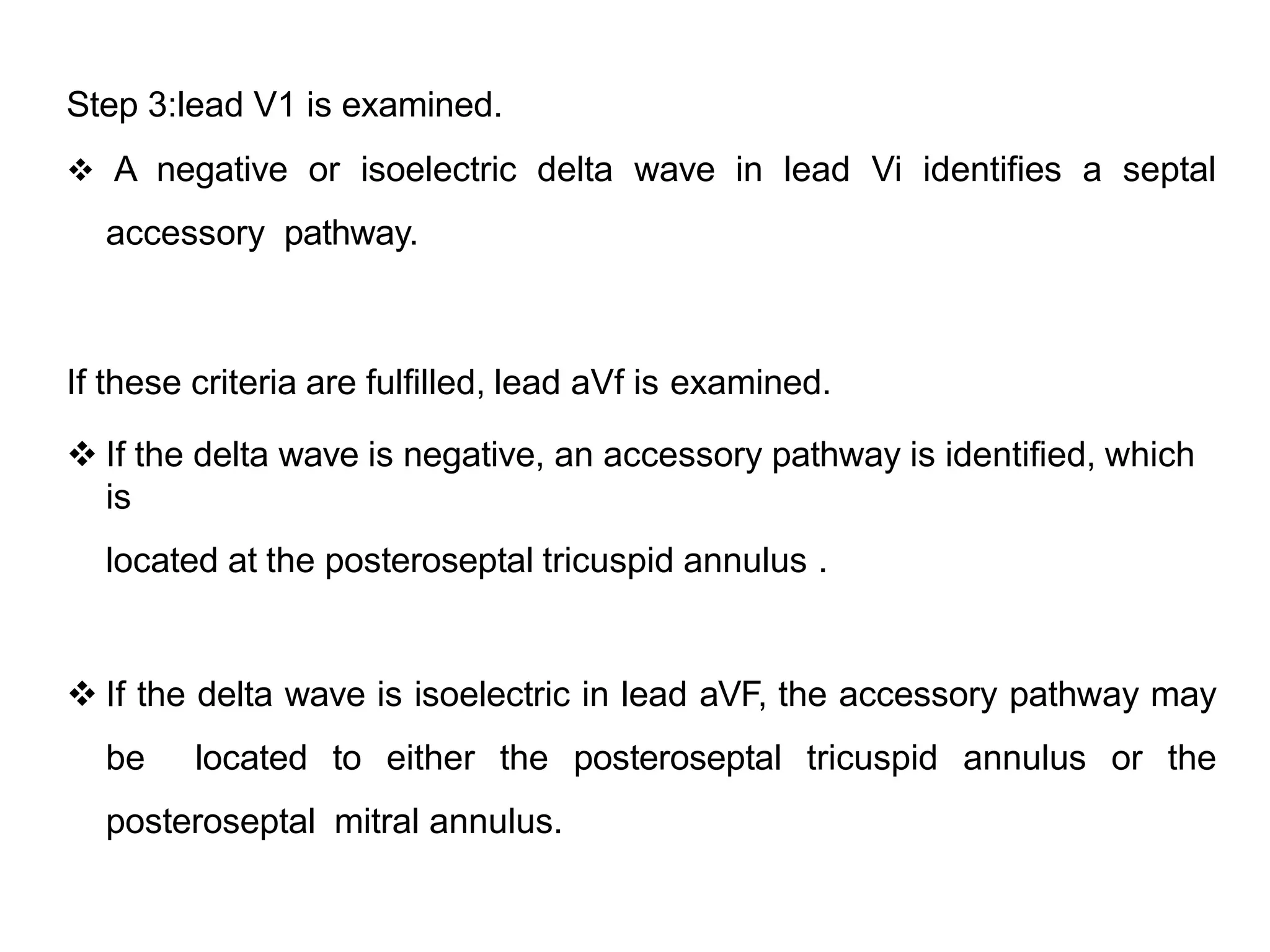
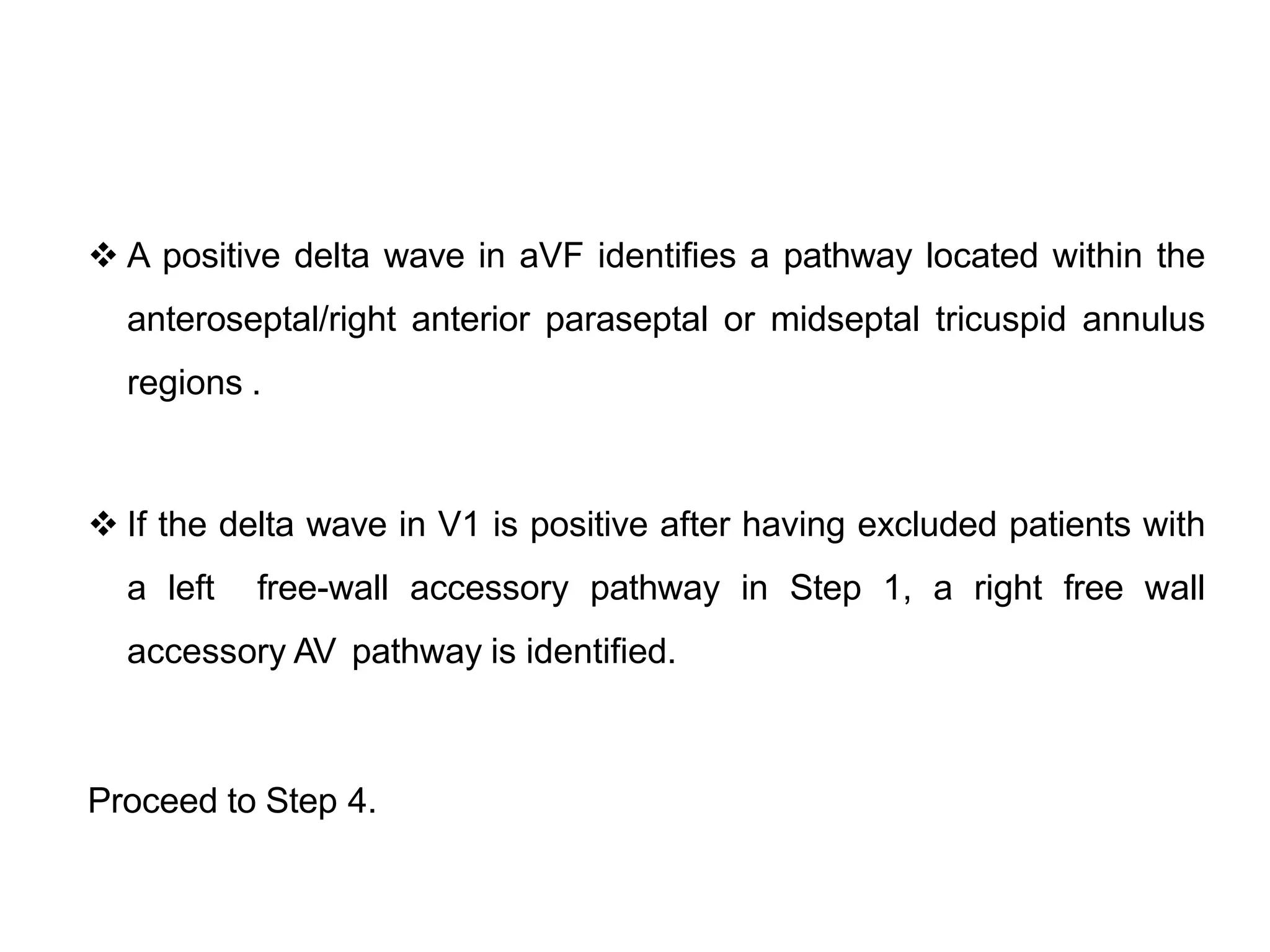
- Factors like precordial transition, delta wave polarity in various leads, and retrograde P wave morphology can provide clues about left vs. right, septal vs. free wall, and anteroseptal vs. posteroseptal localization.
- Accurate localization guides patient counseling on ablation risks and assists planning the procedure